


An Important Debate: Should the Elderly Receive the "Vaccine"
An insider's view into what real scientific discussion should look like.

Dr. Martin Kulldorff is a professor of medicine, biostatistician and epidemiologist that used to teach at Harvard and is one of the authors of the Great Barrington Declaration. Dr. Kulldorff rightly opposed the “vaccination” of children, lockdowns, and masking. He has been instrumental and pushing back against biomedical tyranny, except that he is dead wrong in his belief that “vaccinating” the elderly is somehow beneficial, despite the actual data proving otherwise.
The below exchange between my dear friend and colleague (C) and a well-regarded doctor (MD) is an important series of points regarding “vaccination” and the elderly. It is especially germane to establishing that these “vaccines” are for any demographic identical; that is, these gene “therapies" are undeniable slow kill bioweapons.
The below debate is presented without any edits, exactly as it appeared in the med discussion-only C21 forum thread:
C: Martin Kulldorff is great BUT he states that elderly should take the shots--ignores the early Rx which is available and cures.
not only that, but the legacy studies did not include them and thus we have no research data that properly 'excludes harms' to them and shows definitively, the efficacy or effectiveness. So Martin I love, superb intellect, but he bypasses me with that. I confess. I DONT agree.
I tweeted to them four statements I made to group up friends who do not have a background in biological sciences that were put in layman's terms, suggesting that these injections are inappropriate for any age group and asked for their comments.

DR: I think the group should be very careful about statements regarding age 80 and over patients. Your 4 statements are accurate, but those are reasons why the vaccine might not help rather than evidence that the vaccine did not help.
The UK all cause mortality data DOES show higher mortality in unvaccinated people age 80 and over with around 10 vaccinations necessary to prevent 1 death per month. The vaccine was associated with a benefit in older patients. Now, these results were predicated on existing practices. Would the results have been different had there been widespread use of ivermectin early on in treatment of older patients? We will never know since it was not done. The all cause mortality data DOES show a convergence of mortality between the vaccinated and unvaccinated groups after May 2021 and especially during 2022, so the duration of benefit of vaccination does appear to be only a few months.
We cannot assess the efficacy of most recent boosters on all cause mortality in the elderly because very few people in the oldest age groups stopped the process without getting ALL the shots.

The UK data shows a net HARM or increase in all cause mortality in the vaccinated vs. unvaccinated for age less than 40. We should focus on this message which is supported by the best data we have. The elderly should be counselled that there are significant risks to being vaccinated as well as significant risks to NOT being vaccinated. Each person will need to decide which risks are of most concern.
C: When I have looked at rare sources of age-stratified data by injection status, the elderly do not benefit from this injection. The more injections the more the immune system is destroyed as per Dr. Sabine Hazan et al. Data like this appears to support that conclusion.

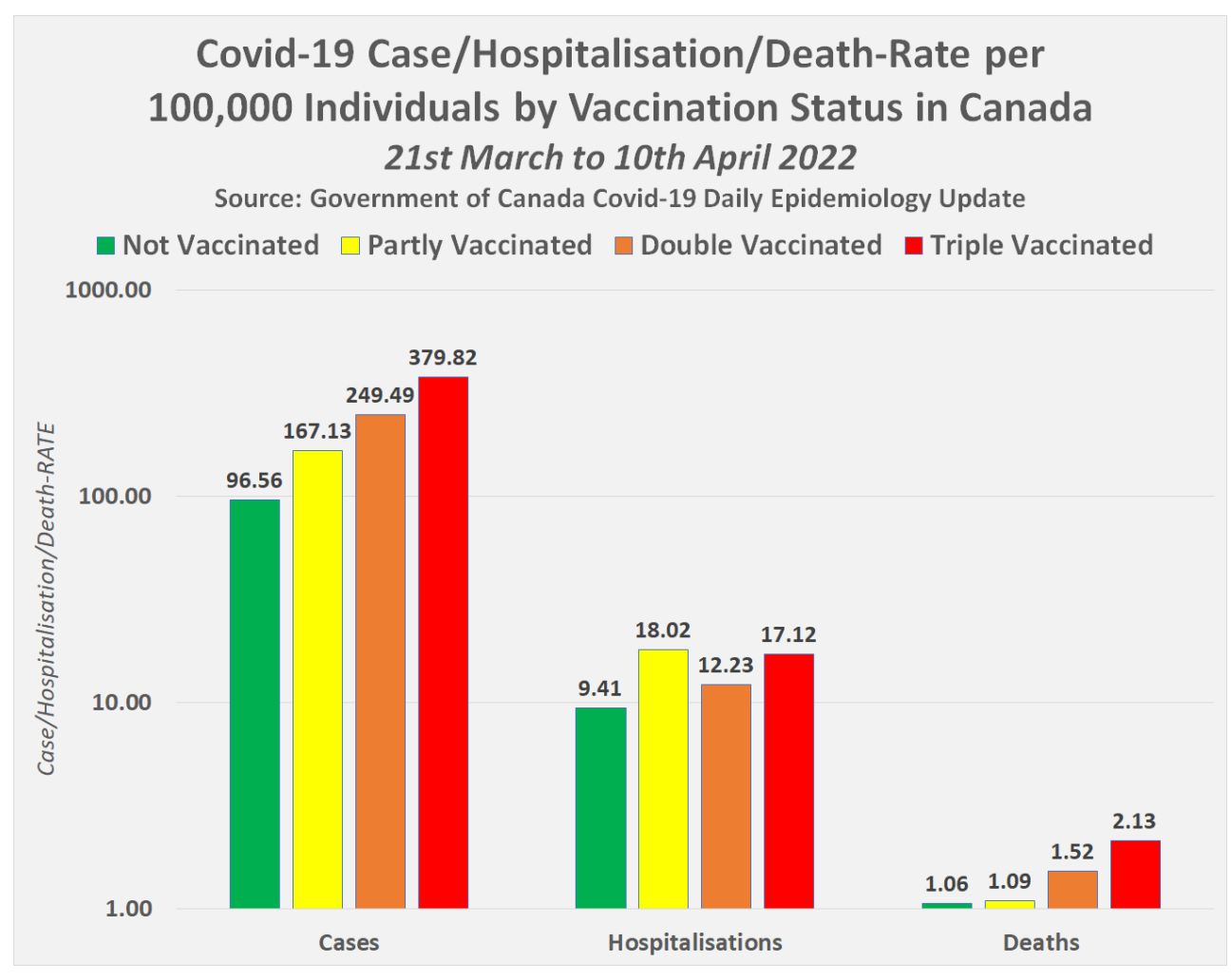
The British Columbia data I posted was in support of Dr. Hazan's position that mRNA injections are destructive of the immune system. The point is that in all age groups and in particular, the elderly more injections they have the worst off they are in terms of mortality. Here is Canadian data that shows the same thing in terms of mortality rates that you speak of but it is not age-stratified.
The more injections the more the immune system is destroyed period!
DR: I think the graph is consistent with some kind of immune suppression effect of the vaccine. The mechanism may be that vaccine interferes with normal immune system development. It could be that the vaccine does nothing for T-cell and IgA immune response.
However, here is how the mainstream is reporting the same data. The case rate for triple vaccinated is almost 4 times the case rate for unvaccinated. The hospitalization rate for triple vaccinated is only 2 times the hospitalization rate for unvaccinated, so the PER CASE hospitalization rate for triple vaccinated is reported as 50% of the PER CASE hospitalization rate for unvaccinated. Likewise, the PER CASE mortality rate for triple vaccinated is reported as 50% of the PER CASE mortality rate for unvaccinated.
With a complicated situation, you can reach any conclusion you want to reach if you selectively report only results that are favorable to one's position. That is why, in my opinion, analysis should start with the most important outcome -- mortality -- and analyzed the ENTIRE population to encompass ALL factors rather than looking at cherry picked subsets which ignore important factors about how/why individuals ended up in particular subsets.
C: The population MUST be stratified by Age Group as people cannot choose their age by behavior. Furthermore, Age Group is the most important factor in determining all cause mortality and COVID mortality.
We need to understand EVERY trick in the mainstream playbook to aid the effort by the AG of Florida to comprehensively evaluate the vaccine. Unlike NEJM, we will have the opportunity to expose the flaws in the mainstream argument.
Would this satisfy what you are looking for?
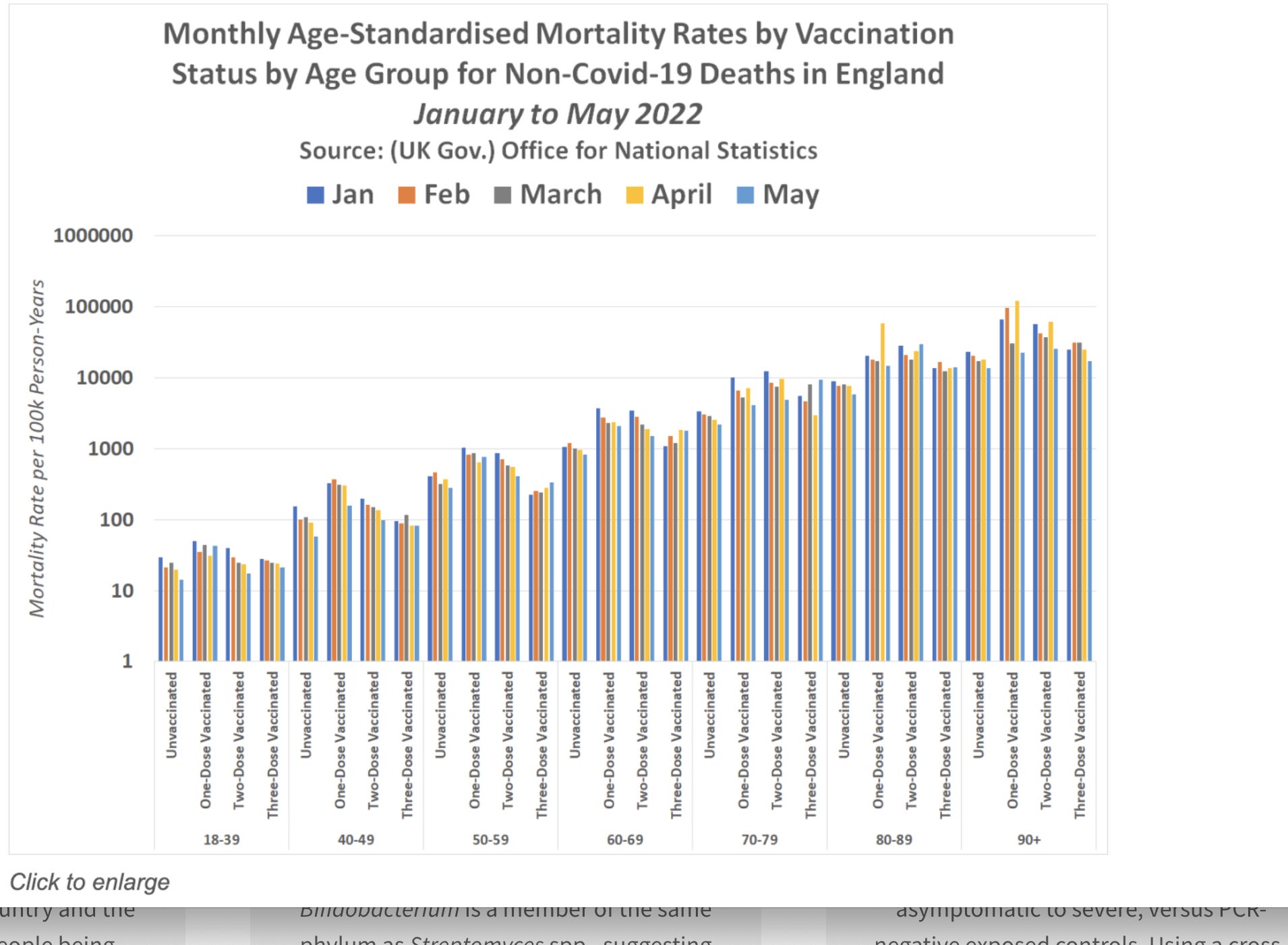
DR: So, for every single age group, the unvaccinated fared better than those with one or two vaccines, and for those over the age of 60, the unvaccinated also fared better than those who had received a booster.
During the time frame of Jan - May 2022, there were very small differences between mortality rates for vaccinated and unvaccinated (follow the thread back to my graph). The big differences were during Jan - Apr 2021. In the earlier time frame, unvaccinated did better than vaccinated for the 18-39 age group, but vaccinated did better than unvaccinated for the older age groups with the number to vaccinate to prevent 1 death/month decreasing from 1,800 for 40-49 to 10 for 90+.
For the time frame pictured in this most recent graph in the thread, any differences between vaccinated and unvaccinated are very small for all age groups as the trends have converged over time.
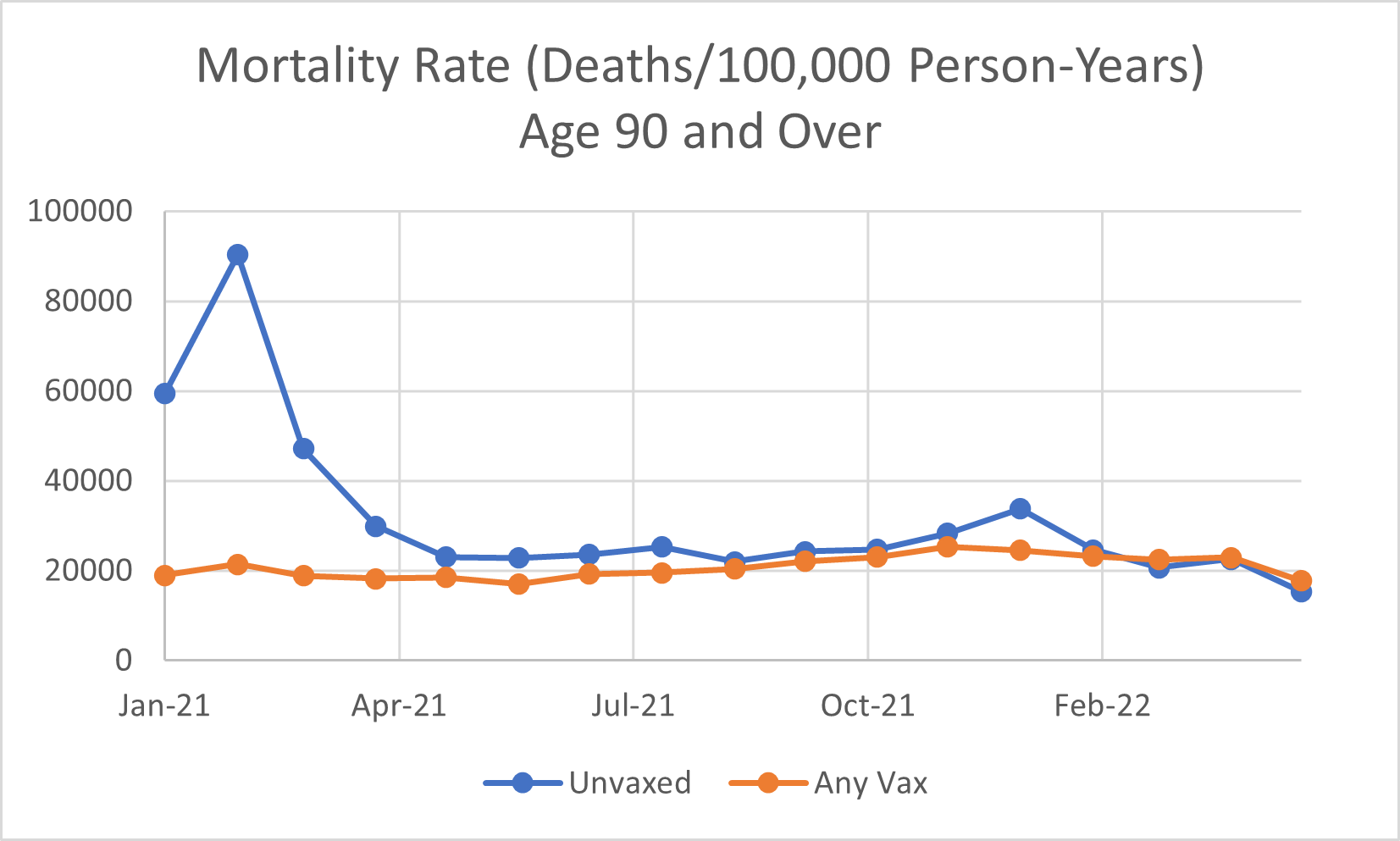
C: The most recent graph in the 80-89 and 90+ cohorts shows significant differences between the unvaccinated and vaccinated for the months from January through May 2022 in favor of being unvaccinated. Your graph puts the vaccinated at a small advantage from January to March 2022. Is the data source I provided different from the one you used?
I suspect that not defining those injected within the first two weeks as "unvaccinated" throws off the results and skews the data in favor of the vaccinated group. The evidence that these injections overtime destroys the immune system is significant but is more of a slow-kill bioweapon hence the results over time do not show convergence but divergence as demonstrated by the most recent graph.
DR: Very small differences for 2022. Big differences for Jan - Apr 2021. Any vaccination mortality was slightly higher than unvaccinated mortality for 90+ during Mar - May 2022.

C: Check it out, my data shows that for the 80-89 group, the unvaccinated ALWAYS are lower than the vaccinated. Your graph for the 80-89 group shows the opposite.
Month by month, it is very consistent on my graph that one is ALWAYS lower than the other. Something is wrong, but one thing I know for sure, it is not in my data.
As someone else mentioned in the thread, this argument is not relevant as the unvaccinated as designated as COVID+ that died in the UK in 2021 were murdered through medical malpractice ending with "sedation" with Midazolam. They were not given valid early treatment protocols that saved hundreds of thousands of patients' lives, thanks to many members of this group.
This is not unique to the UK as I witnessed the murder of my own Father In law (effectively my adoptive father of 40 years as I lost father very young) with this "MAID" in Canada protocol ending with a Midazolam injection. I happened to walk in when the nurse was administering the midazolam injection, but it was too late. I called in the physician and told them that they had just administered a lethal injection
and showed them on my Iphone that Midazolam is part of the Medically Assisted In Dying Protocol (MAID) administered without the patient consent. This was after they tried to argue that MIdazolam was not that.
They had been pressuring my Father In law for over a month to kill himself, but I digress.
If you don't believe me that it is the same in the UK here is the evidence. Keep in mind that NG163 clearly states, Midazolam did not have a UK marketing licence to be used for breathlessness or agitation at the date of its publication. If prescribed for the same, it would therefore be regarded as being used off label. A PowerPoint presentation created by Clare Wills Harrison (see here) explains the extra requirements placed on anyone prescribing a medicine off label. As mentioned for the US you should also consider the consistent refusal by the UK health agencies to allow prescribing off label for other cheap anti-viral drugs to treat Covid.
Thirty-four percent of people working in health and/or social care in the UK said they were under pressure to put DNACPR’s in place without involving the person. In addition, 71% of advocacy organizations and campaigners said they experienced DNACPR orders put in place or pressure to make them without being involved in the decision. And those DNACPR orders were wrongly used as an excuse to begin end-of-life care. This according to the Care Quality Comission Investigative report https://www.cqc.org.uk/sites/default/files/20201204%20DNACPR%20Interim%20Report%20-%20FINAL.pdf
The National library of Medicine has this article in its archives regarding Midazolam. "Midazolam injection may cause serious or life-threatening breathing problems such as shallow, slowed, or temporarily stopped breathing that may lead to permanent brain injury or death. You should only receive this medication in a hospital or doctor's office that has the equipment that is needed to monitor your heart and lungs and to provide life-saving medical treatment quickly if your breathing slows or stops. Your doctor or nurse will watch you closely after you receive this medication to make sure that you are breathing properly." https://medlineplus.gov/druginfo/meds/a609014.html
So can the UK Government explain why the “NICE Document” published in April 2020 instructs doctors to treat Covid-19 patients with Midazolam, and why during the same month out of hospital prescribing for Midazolam was twice the amount seen in 2019? A practice that to this day has not ended and certainly continued on a larger scale throughout 2021 compared to 2022 where these wretched protocols are finally being exposed to a wider audience than medical professionals.
To suggest to this group that these injections were ever useful to any age group is nonsense and your data from 2021 does not support it, as there are too many confounding factors, not the least of which is eldericide of the unvaccinated.
As stated repeatedly, what you are seeing in 2022 is the result of gradual immune system destruction, a more subtle way of mass murder.

DR: "Check it out, my data shows that for the 80-89 group, the unvaccinated ALWAYS are lower than the vaccinated. Your graph for the 80-89 group shows the opposite.
Month by month, it is very consistent on my graph that one is ALWAYS lower than the other. Something is wrong, but one thing I know for sure, it is not in my data. "
These differences are very small and look like noise.
"As someone else mentioned in the thread, this argument is not relevant as the unvaccinated as designated as COVID+ that died in the UK in 2021 were murdered through medical malpractice ending with "sedation" with Midazolam. They were not given valid early treatment protocols that saved hundreds of thousands of patients' lives, thanks to many members of this group. "
As I said when I first got into this thread, the all cause mortality data reflect existing practices. The results might very well have been different had different protocols been used. However, different protocols were NOT used, so we will never know what would have happened. Your argument is an emotional argument rather than a scientific one. Good luck with that in a hostile court of law.
Believe it or not, I am on your side, but I want to affect real change given the facts that we are dealing with a hostile mainstream, a hostile government, and hostile courts. Look at the title of the thread. An eminent person (Kulldorff) states elderly should get the vax. Feel free to disagree with that person, but the hostile judge is going to agree with Kulldorff. We can change current recommendations for people under the age of 40 right now. Maybe we can change the recommendations for the elderly a year from now, but don't overplay your hand.
C: "These differences are very small and look like noise."
Sigh....


DR: For the 80-89 and 90+ age groups, there are very few patients in the One-dose and Two-dose groups. The Three-dose > 21 days subgroup is over 90% of the the patients in the age group making the other vaccination subgroups pretty much meaningless.
You can make any difference look like a large amount when you take away the frame of reference. If you want to ignore the data from Jan-Apr 2021, be my guest, but the data will not go away just because you exclude it from your graph.
C: "For the 80-89 and 90+ age groups, there are very few patients in the One-dose and Two-dose groups. The Three-dose > 21 days subgroup is over 90% of the the patients in the age group making the other vaccination subgroups pretty much meaningless."
Even comparing the unvaccinated group to the three dose only vaccinated group the numbers are not even close with the single exception of January 2022 in the 90+ group where the difference is likely not statistically significant albeit the unvaccinated group is not worst off than the vaccinated group.
"You can make any difference look like a large amount when you take away the frame of reference. If you want to ignore the data from Jan-Apr 2021, be my guest, but the data will not go away just because you exclude it from your graph."
Below is what the vaccine rollout looked like in 2021 https://en.wikipedia.org/wiki/COVID-19_vaccination_in_the_United_Kingdom#/media/File:Graph_of_first_doses_as_of_30_may_2021_UK_Vaccines_COVID.png
So from January 2021 to February 2021 very few were vaccinated and that is precisely where the spike is. By the way in your definition of the data of vaccinated does it include those that were injected in the first two weeks? The same issue you are attempting to point out in the 2022 data is even more distorted in 2021 except the vaccinated group is very small.
Secondly, I am suggesting as is evidenced of Dr. Hazzan et al the worst part of the vaccine is the destruction of the innate immune system that manifests itself slowly and indeed the 2022 data I have shown clearly supports that hypothesis.
Again, what is the source of your data? Your 2022 numbers are not even remotely close to mine. Science is about reproducible data and I can't reproduce yours.
I am hoping we can convince Dr. Kulldorff that his take that these injections are beneficial to the elderly is incorrect BEFORE the Grand Jury is impaneled in Florida. During the panel discussions, he labeled those that take this view as "extremists" that are not helpful to our cause.
I agree with you that anecdotal/emotional evidence is not helpful and the good news is the statistical data I have presented is solid and trying to represent it as something other than it is is not helpful and that cuts both ways!

Ok thanks, even with that outside of immediate adverse events it would take 5 months + for the harm to the immune system to manifest itself As your chart shows for the first four months of 2021 you see the unvaccinated have a much higher mortality rate than the vaccinated.


Subsequent to August 21 2021 the unvaccinated in all age groups have the lowest mortality rate and that is very evident in the elderly group we are discussing from 2022 onwards.
It is totally understandable why Dr. Kulldroff thought the vaccines were beneficial to the elderly. Unfortunately, the harms take time to manifest themselves but the data where it is all over the world.
Canada, UK, and New Zealand show the same pattern.
I do not think it is unreasonable to have this discussion with Dr. Kulldroff and get his take on this data. The developers of these products designed the spike protein to induce every disease you can imagine.
The Furin cleavage site was ALWAYS omitted in previous vaccines HIV, RSV etc and their are even videos from 2014 with Pfizer developers saying they always omit this site. In 2015 Moderna patents this sequence and makes sure that the mRNA codes for this spike protein were replete with this harmful insert and of course they did not miss a beat and included the HIVGP120 insert that has very similar harms to the Furin Cleavage site.
When you look at the totality of the evidence there was no altruistic goal in the development of these injections. We all know this. So you are saying how do you sell this to the misled public who my not know how to assess scientific evidence? The answer is clear, we need to convince people like Dr. Kulldroff that we speak the truth.
DR: That was a very nice summation of the data by C and I will leave A (2SG: A is another longstanding C19 group member) with the last word.
C: BOOM, A in on the money here. It is not a vaccine and it is simplistic to just conclude this when we have early treatment but key is that data shows us the 3rd and 4th shot to elderly is lethal.
I need someone to show me data where this works and while you do it, please show me how you adjust for early treatment, natural immunity and also co-morbidities across comparative groups.
A: No one can DR. It does not work when all those you list are taken into account---natural immunity WORKS and all the rest is mere poison and bureaucratic abuse engineered by the bureaucrats, big tech, and unfortunately most of our colleagues who lack or do not know how to use critical thinking skills---IQ does not matter but simply helps with their denial in front of patients who inquire.
The above debate was forwarded directly to Florida’s Surgeon General Dr. Joseph Ladapo ahead of Governor Ron DeSantis’s crimes against humanity investigation:
Many of the points in the above debate will more than likely be presented to the grand jury.
Do NOT comply.











I’ve been saying this for a long time. I’m no doctor or scientist! I’m a high school grad. What I have is common sense (a lot of street smarts too). The jab is not safe or effective...for anyone!!!!!!
There has been a lot of discussion on this lately around various Substacks. Thank you for reiterating the importance of this...not just for Covid jabs, but for ALL vaccines like flu, etc.
I mean, really, how hard is it to understand that if you are old, your immune system is crap.
You cannot make an old horse pull a heavy cart..it will drop dead in its traces.
Maybe if they concentrated on things that could improve /delay the onset of senescence in your immune system of thymus BEFORE YOU GET TO THIS POINT, we would all be better off.
Signed, An Old Lady.
PS if anyone has any natural ways you might stop your thymus from further deterioration, please feel free to suggest!