In a world reeling from the consequences of the PSYOP-19 scamdemic, where trust in institutions is at best hanging by a thread, a growing body of evidence has emerged that shatters the very foundations of medical integrity.
This is not hyperbole, this is a wake-up call.
The supposed “failure” of ivermectin, a repurposed Nobel Prize winning drug that could have saved millions of lives during the height of the “pandemic,” has now been exposed as the result of a meticulously orchestrated Medical Industrial Complex campaign of deceit, fraud. and, ultimately, mass murder.
There is a war being actively waged against humanity by these architects of deception and bioterror who undermined one of the most affordable and potentially life-saving treatments during their “pandemic.” The curtain has been pulled back, and the evidence is irrefutable.
Investigators of the TOGETHER, COVID-OUT, ACTIV-6 400, and PRINCIPLE trials have engaged in actions so unethical, so insidious, that their criminal actions should send shockwaves throughout the medical community, and the world at large.
The Case Against the Trials: Unveiling the Fraud
Dr. Michael Goodkin, alongside renowned medical experts such as Drs. Pierre Kory, Peter McCullough, and David Wiseman, has painstakingly laid out the evidence. They aren’t wild-eyed conspiracy theorists or fringe actors—they are highly credentialed professionals who have dared to expose what can only be described as one of the largest medical cover-ups in modern history. They have meticulously examined the data from these trials, and the findings are nothing short of explosive.
The fraud began with the deliberate underdosing of ivermectin. While the Front Line COVID-19 Critical Care Alliance (FLCCC) recommended much higher doses, these trials used significantly lower amounts. In some cases, as much as 43% less than what was considered necessary for effectiveness. Even worse, ivermectin was administered on an empty stomach, a fatal flaw in protocol, as this reduces the drug’s absorption by over 150%. How can such a glaring oversight be anything but intentional?
But it doesn't stop there.
The investigators in these trials also knew that ivermectin was being administered far too late to be effective, often 5-6 days after the onset of symptoms.
Timing is everything when it comes to antiviral treatments, and administering a drug too late is akin to sabotaging the trial from the start. And sabotage is exactly what happened.
Changing the Rules Mid-Game: Manipulating Endpoints
One of the most egregious acts of fraud came in the form of manipulating the primary endpoints during the trials. For instance, in the ACTIV-6 400 trial, ivermectin showed a remarkable 98% chance of benefit at the original 14-day endpoint. What did the investigators do? They moved the goalposts, extending the endpoint to 28 days, reducing ivermectin statistical benefit to 91%, thus declaring it ineffective.
Let’s be clear: even a 91% chance of benefit would make any reasonable doctor prescribe the treatment; yet, they dismissed it.
This wasn't a mistake—it was a deliberate act to suppress the truth.
A Coordinated Effort to Hide the Truth
The deception didn’t end with dosing and timing.
The trials were also designed to lump together data from different COVID-19 variants, ignoring the fact that ivermectin was shown to be highly effective against the delta variant, but not omicron. By failing to report variant-specific data, the trials masked ivermectin efficacy during the critical delta surge, which dominated from mid-2021 to late 2021. Investigators knew this but chose not to disclose it.
The ACTIV-6 400 trial is a prime example of this. It began with over 90% of patients infected with delta, where ivermectin proved beneficial. Yet, as omicron emerged and ivermectin efficacy waned for that variant, the investigators continued to enroll omicron patients—contrary to the trial's protocol—and combined the data to dilute ivermectin's proven effectiveness. This isn't science; it's a scam.
Who Benefits? Follow the Money
Who stood to gain from discrediting ivermectin? As usual, follow the money.
Bill Gates, a major sponsor of the TOGETHER trial, made $500 million on Moderna stock. The pharmaceutical giants stood to profit immensely from pushing high-priced treatments like Paxlovid, which cost hundreds of dollars per patient, while ivermectin—at just $20—could have saved millions of lives. This wasn't just about health; it was about protecting profits, no matter the cost to human life.
The Role of Academic Medicine: A Culture of Silence
Academic medicine did not just fail; it colluded in this fraud. Major institutions, including the NIH, NIAID, CDC, and universities involved in the trials, have been implicated. Hundreds of academic physicians were notified about the problems with the trials, yet none spoke up.
Why?
Fear of losing funding, reputational damage, and reprisals from the federal government. This cowardice has resulted in global consequences, affecting billions of people.
Time for Action: Demand Accountability
This is a call to arms for every doctor, every patient, every citizen.
The fraudulent actions taken in these trials must be exposed. ivermectin, had it been properly tested and administered, could have changed the course of the pandemic. Instead, millions were left to suffer, while academic medicine, government agencies, and pharmaceutical companies reaped the rewards by pushing their slow kill bioweapon “vaccines” which did absolutely nothing to prevent transmission, nor attenuate symptoms all while genetically modifying the recipients into walking spike protein factories afflicted with VAIDS and the associated severe adverse events, not limited to surging excess mortality rates as a function of the “Safe and Effective” EUA interventions.
We must demand transparency. We must demand that the raw data from the ACTIV-6 400 trial be subpoenaed and reviewed. The global public deserves to know how these trials were manipulated, how the truth was hidden, and how lives were lost for profit.
This isn’t just about ivermectin. This is about holding accountable those who have abused their power to control medical narratives and shape public health policy in ways that prioritize profits over people.
The War Has Just Begun
This battle is far from over.
Dr. Goodkin and his colleagues are not backing down, and neither should we.
We must call for full investigations, demand the truth, and ensure that those responsible for this medical fraud face justice. The time for complacency is over. The time for action is now.
This is a declaration of war—a war on the fraud, corruption, and unethical behavior that has permeated our medical institutions during one of the greatest manufactured health crises in history.
The truth will come out, and when it does, those responsible will be held to account.
The question is: will you stand with us?
Will you stand for the truth?
The following is the video transcript:
Problems With the Large Randomized Ivermectin Trials
Michael B. Goodkin MD, FACC
Moderator: Hello. We have Dr.. Michael Goodkin with us today to go over data which he believes shows unethical actions by the investigators of the 4 large randomized ivermectin trials which falsely made ivermectin appear ineffective. Dr. Goodkin, why don’t you tell us something about yourself.
Goodkin: I’m a retired private practice noninvasive cardiologist living near Philadelphia. Along with Drs. Pierre Kory, Peter McCullough and David Wiseman, I’m on the medical advisory panel of Trialsite News where I’ve written many opinion pieces on what I perceived to be unethical behavior by the government and many investigators in regards to repurposed drugs to treat COVID.
Moderator: You told me you have published very little. Are you concerned about your credibility given that you were not in academic medicine?
Goodkin: Those in academic medicine will feel the lack of academic credentials is important but my academic credentials are irrelevant.
The only thing that matters is the data from the published trials and if my analysis is accurate. All of these trials have been vetted by others with high levels of competence in trial analysis.
They found many problems in these trials. I used their work, especially that of Dr. Pierre Kory, found some new things in the NIH sponsored ACTIV-6 400 trial and found some new ways to present the data so that physicians and the public could understand what happened in those trials.
Unlike heavily credentialed “experts”, I am not being paid and have no conflicts of interest. Those in academic medicine want to protect the reputation of academic medicine. We will see that academic medicine was involved in some terrible deception and cowardice. I have nothing I want to protect other than the health of Americans.
Moderator: What are you going to be speaking about today?
Goodkin: I’m mainly going to speak about the deceptive actions by the investigators of the TOGETHER, COVID-OUT, ACTIV-6 400 and PRINCIPLE ivermectin trials. First I will give an overview of the problems in those trials, then I will speak about how our government did nothing with mast cell activation syndrome, the treatment of which would have been very helpful especially early in the pandemic. Lastly, I will go into great detail about how the 4 trials were conducted using charts and diagrams.
Moderator: Why don’t you get started.
Goodkin: There was a great deal of deception in the large randomized ivermectin trials, TOGETHER, COVID-OUT, ACTIV-6 400 and PRINCIPLE. This document shows that deception using evidence directly from the 4 large randomized ivermectin trials:
(1). Ivermectin was severely underdosed, given on an empty stomach when the blood level of their average 30 mg. dose would have been 157% higher if given with a fatty meal and ivermectin was given late, at an average of 4.9 days in the 4 trials.
(2). The doses were very low in the trials. Guzzo et al.(8) had shown ivermectin to be safe and well tolerated at 120 mg. daily for 3 days. TOGETHER was using about 30 mg daily for 3 days.
(3). The NIH sponsoredACTIV-6 400 trial claimed to be using the same dose as TOGETHER. That meant if TOGETHER failed to show benefit, ACTIV-6 400 would be repeating a negative study. It turned out worse than that. ACTIV-6 400 repeated the TOGETHER trial with a lower dose of ivermectin.
TOGETHER announced 8/6/21 that ivermectin failed to show statistical benefit. ACTIV-6 400 should have started all over again with those randomized to ivermectin getting a much higher dose. At the least they should have added a high dose arm. Instead, they randomized over 1400 more patients to placebo or an average 343 mcg/kg for 3 days, a LOWER dose than the approximately 380 mcg/ kg for 3 days which TOGETHER had used and which had failed to show benefit. Crazy.
(3). In October 2021 when about half the patients had been enrolled, Drs. Francis Collins NIH chairman, Cliff Lane, deputy chairman of NIAID, Susanna Naggie, ACTIV-6 principal investigator, Carolyn Bramante, principal investigator of COVID-OUT and WCG IRB, in charge of patient safety in ACTIV-6 400 were emailed that they had 99% delta, that they were giving patients 40% of the FLCCC recommended dose and that they were giving ivermectin on an empty stomach when the blood level of their typical 30 mg dose would have been 157% higher if given with a fatty meal.
Dr. Lane said they were looking into it. The ACTIV committee reviewed it but no changes were made, leaving those randomized to ivermectin undertreated.
(4). Ivermectin showed a 98% chance of benefit, statistically significant, at the original primary endpoint of 14 days but the investigators unethically changed the primary endpoint during the trial to a ridiculous 28 days causing ivermectin to have only a 91% chance of benefit, declared it ineffective and said it should not be used. Anyone would gladly take a drug with a 91% chance of benefit rather than get no treatment.
(5). An analysis of the combined trials showed that ivermectin was beneficial for delta and ineffective for omicron in ACTIV-6 400, which would have easily been seen in real time as the trial progressed. The investigators in COVID-OUT and TOGETHER, which were running concurrently had to see the same thing and didn’t report it over the 5+ months when delta dominated.
By combining the data from the 3 trials ivermectin would have been declared beneficial by the end of September and millions of patients could have been treated with ivermectin until omicron came in mid December.
6). By combining the delta data from ACTIV-6 400, COVID-OUT and PRINCIPLE or from the ACTIV-6 400 alone, ivermectin would have been deserved to be declared effective and an emergency use authorization and would now be in use for omicron like paxlovid and molnupiravir which got EUAs based only on data in delta patients then were used for omicron without randomized trial data showing benefit for omicron.
7). None of the 4 trials made any attempt to look at ivermectin's effectiveness for the different variants. All 4 trials lumped the patients with different variants together. There was no reason to think that ivermectin would be equally effective for delta and omicron, the dominant variants in COVID-OUT, ACTIV-6 400 AND PRINCIPLE. By assuming delta and omicron were equally effective they were able get away with (8),(9), (10) and (11). If ivermectin was equally effective for delta and omicron, running a trial with a higher dose, enrolling extra patients and not reporting the interim data would not appear to be a problem. Here's what the
investigators did:
(8). In ACTIV-6 400 the study was supposed to go 1200 patients but investigators enrolled an extra 391 omicron patients, against the rules of the protocol. Those patients had almost no benefit. The addition of them to the 1200 patients the investigators were supposed to enroll lowered the statistical benefit of ivermectin substantially. Unless you knew that ivermectin was beneficial for delta and not omicron, one would never know there was anything wrong.
(9). Of the first 924 patients, over 90% had delta for which ivermectin was effective. In ACTIV-6 400 the investigators didn't report any of the interim data every 300 patients they were supposed to report because they knew that ivermectin showed benefit at 900 and probably 600 patients. Had delta and omicron been equally effective this wouldn't have mattered.
(10). The investigators ran the ACTIV-6 600 trial in 95% omicron patients, knowing that ivermectin would not show benefit when given at 5 days of symptoms because they had seen ivermectin’s lack of benefit for omicron in the ACTIV-6 400 trial.
(11). In an editorial in JAMA Network, JAMA editor in chief, Dr. Kirsten Bibbins-Domingo implied to readers that the failure of ivermectin in ACTIV-6 600 that ivermectin had not failed in earlier trials due to underdosing when in fact ACTIV-6 600 had treated 95% omicron and ACTIV-6 400 had treated over 50% delta patients where ivermectin was known to be effective. Apples and oranges. Deceptive.
(12). The PRINCIPLE trial claimed ivermectin showed no benefit. In the 400 pages of supplemental data there was clear, highly statistically significant evidence of a 36% decrease in Long COVID.
(13). Had ivermectin been given as recommended by the FLCCC Alliance, ivermectin would have crushed COVID in all 4 trials, ivermectin would have warranted an EUA and been in use today at FLCCC dosing, given as early as possible.
Ivermectin would clearly have been much better than no treatment which is what the vast majority of patients in the world get and possibly as good or better than paxlovid for acute symptoms. It is clearly better than paxlovid for preventing Long COVID for which paxlovid has no benefit. Ivermectin can be made for less than $20 a person compared to over $500 for paxlovid and molnupiravir.
(14). Those patients who enrolled in the ACTIV-6 400 trial, asking to be randomized to ivermectin who actually were randomized to ivermectin should be very upset that the investigators did everything they could to see that they got as little benefit as possible so that they could make ivermectin falsely appear ineffective.
(15). The most depraved use of ivermectin occurred in hospitals where many hospitals refused to allow the use of ivermectin even when ordered by a physician or requested by the family. Hundreds of times hospitals were willing to fight families in court to prevent their critically ill loved ones from receiving ivermectin.
Buffalo attorney, Ralph Lorigo represented 200 families. If he won in court 67 of the 70 patients lived. 3 patients on ventilators for over a month died despite receiving ivermectin. He said that the 130 patients in whom he lost in court or didn't get to the judge in time, all of them died but I found out that one patient's family sneaked ivermectin into the hospital and the patient lived.
(16). Hundreds of academic physicians were notified of the unethical actions of the ACTIV-6 400 trial, including 4 voting members of the independent monitoring committee, numerous physicians where they were employed and 12 physician site directors. The ACP,
IDSA ,AMA and ACC were notified multiple times. No one in academic medicine did anything due to fear of losing their jobs, losing money for their institutions and fear of government reprisals.
Moderator: I’ll be excited to see how you will prove all of that. How did you get involved with ivermectin?
Goodkin: It actually started with my interest in famotidine which blocks H2 receptors on mast cells.
I’m very knowledgeable about POTS and MCAS which are often present in Long COVID. I probably have had MCAS for 30 years and I have Long COVID. My daughter has POTS and MCAS. I saw over 400 POTS patients in my practice. At least 40% have MCAS. I’m on the medical advisory boards of Standing Up To POTS and have a 501c3 charity, Physicians for POTS.
Moderate: Why don’t you tell us how you got involved in MCAS?
Goodkin: In January 2021 I read a great article by mast cell expert, Dr. Lawrence Afrin(22). He suggested that the symptoms of COVID looked like those of mast cell activation syndrome(MCAS). He believes MCAS is present in 15-20% of everyone. He suspected that the patients who were getting really sick were those with abnormal mast cells.
Mast cells are a type of white blood cell which contains a lot of chemical mediators. Mast cells release histamine in response to seasonal allergens but respond to infection by releasing chemical mediators which in the case of COVID, Dr. Afrin felt contributed to cytokine storm.
If his patients who were on prophylactic H1 blockers like Zyrtec and H2 blockers like famotidine(pepcid) got infected, they never wound up in the hospital. The treatments for MCAS are usually generic and over the counter drugs, something drug companies don’t like.
I sent the Afrin article to the American Academy of Asthma Allergy and Immunology(AAAAI) who wrote back that they were excited and were sending my email to the Biden coronavirus task force.
3 weeks later I got an email from AAAAI that what Dr. Afrin said was all theory. I suspected that AAAAI had been compromised. Later I saw videos of Drs. Rochelle Wolensky and Peter Hotez on their site which heightened my suspicions. I have never seen anything on their website suggesting that COVID has anything to do with mast cells.
I sent them a randomized trial of 55 pre omicron COVID patients,(23) averaging 35 years old who got benefit from high dose famotidine. It’s very hard to show benefit in young patients. Paxlovid didn’t work in patients averaging 42 years old in EPIC SR. It seemed very likely that in older, sicker patients famotidine might be of benefit. Neither famotidine or ivermectin were ever tested head to head against the new antivirals. Since famotidine could treat COVID in pre omicron variants and Long COVID in omicron, maybe it would have benefit to prevent Long COVID or to treat those who are not candidates for paxlovid or in whom paxlovid doesn’t work.
From a CNN article about the trial(26), “I’m totally underwhelmed,” said Dr. Carlos del Rio, then president elect of the Infectious Disease Society of America."
“It certainly doesn’t rev my motor,” said Dr. William Schaffner, an infectious disease expert who serves as a vaccine adviser to the US Centers for Disease Control and Prevention. Neither he nor del Rio worked on the study.
“Schaffner and del Rio, the infectious disease experts, said there’s no reason to spend money on a large clinical trial of famotidine, especially because in the US, there are antiviral drugs and a monoclonal antibody authorized to treat early- stage Covid.”
You can get 200 20 mg famotidine pills on Amazon for $10. It would treat 1.5 patients as opposed to paxlovid, $530 and molnupiravir, $700 per patient.
In addition, famotidine showed benefit in those 35 years years old. Paxlovid has been proven not to be of benefit in that age group. It has no randomized trial data showing benefit for omicron patients.
"Dr. Emad El-Omar pointed out that after two weeks, twice as many people who received a placebo remained symptomatic as those who took famotidine.”
“This is impressive!” El-Omar, a professor of medicine at the University of New South Wales Sydney in Australia, wrote in an email to CNN.
Dr. Kevin Tracey, CEO of the Feinstein Institute for Medical Research at Northwell Health asked. “Can we take a safe drug off the shelf, one that could be manufactured [and essentially] given away to countries that have nothing to treat Covid?” “It’s an important question for global health.” The same could be said about ivermectin.
Unfortunately no one did a large study of famotidine or any other mast cell treatments with the exception of an ACTIV group study of leukotriene inhibitor, montelukast, which was given to omicron patients most likely at 5 days of symptoms when nothing works well. The study was worthless.
Every Long COVID expert I know of says that the majority of Long COVID patients have MCAS which sometimes responds to very simple over the counter or generic treatments.(25)
I began to listen to Dr. Pierre Kory about ivermectin. He testified to the senate and the FDA. He showed a lot of trials and meta analyses showing benefit.
When I saw that 4 large randomized ivermectin trials were beginning in 2021, the first thing I noticed was that the dosing in all the trials was about the same and lower than that recommended by the FLCCC Alliance who from what I saw were top ivermectin experts in the world.
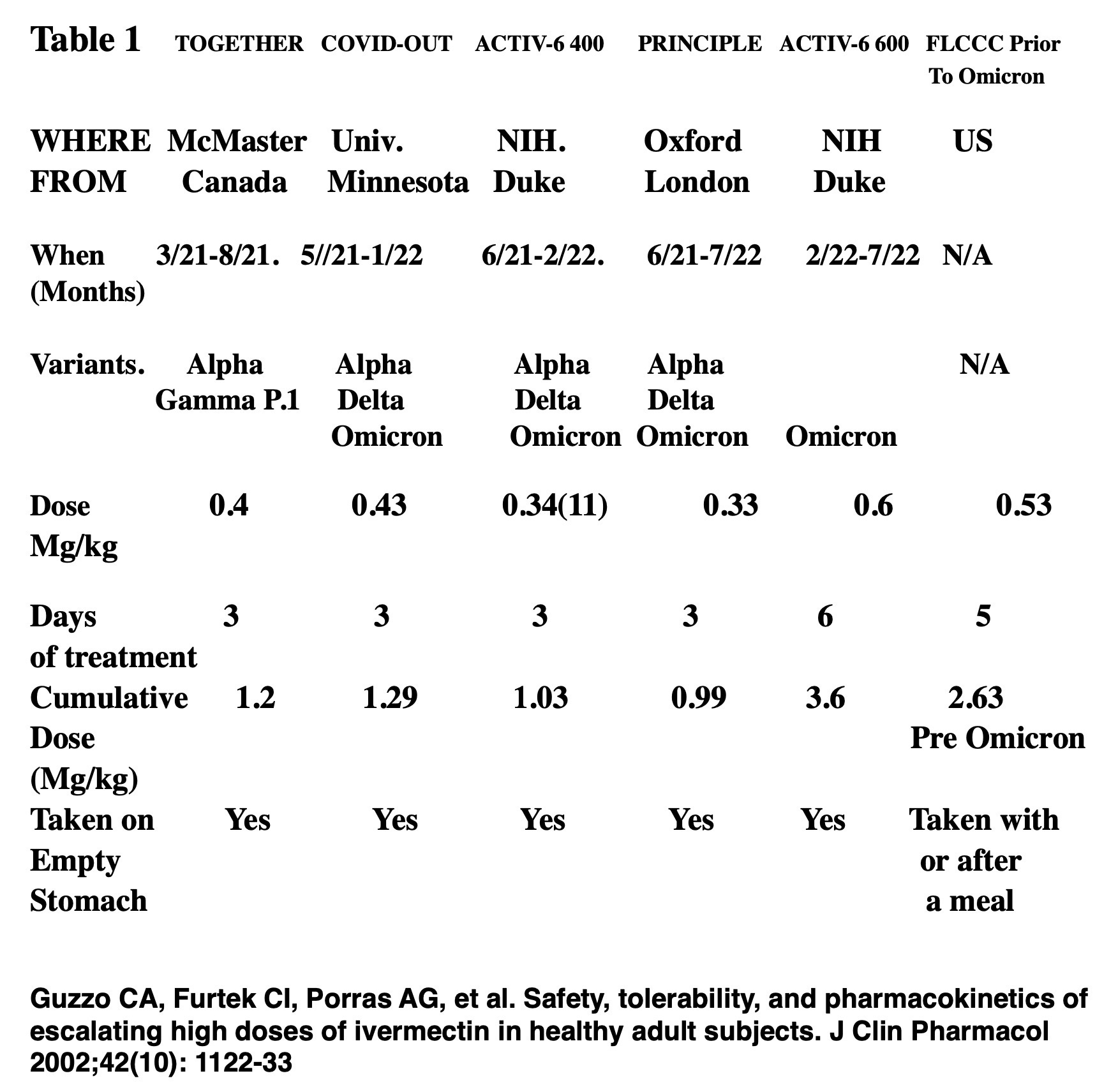
Table 1 shows the dosing, results and timing in the 5 large randomized ivermectin trials and FLCCC recommended treatment during ACTIV-6. (1)(2)(3)(4)(5)
Ivermectin safe and well tolerated to 120 mg daily for 3 days. 2. Ivermectin blood level 157% higher after a fatty meal.
Ivermectin blood level 157% higher after a fatty meal.
WHAT DID WE LEARN FROM PAGE 1?
1) The 4 randomized trials which started prior to omicron started within about 3 months of each other.
2) They used within 23% of the same cumulative dose of ivermectin, quite a coincidence.
3) The average cumulative dose of 1.11 mg/kg was 43% of the average cumulative dose recommended by the FLCCCAlliance, 2.63 mg/kg during that period.
4) Guzzo et al.(8) said that 120 mg daily for 3 days was safe and well tolerated. The average dose of ivermectin in the 4 trials was about 30 mg for 3 days. There is lots of other data showing the safety of ivermectin at even higher doses.
5) All 4 trials which began prior to omicron gave ivermectin on an empty stomach.
6) Guzzo et al. said that a 30 mg dose when given with a fatty meal has a 157% higher blood level. There is no data on the safety of higher dose ivermectin given with a fatty metal for multiple days but the experience of those who use it that way is that it’s very safe.
7) COVID-OUT, ACTIV-6 400 and PRINCIPLE all had some alpha to start then treated predominantly delta then omicron.
8) ACTIV-6 400 2nd author, Dr. David Boulware discussed dosing with Dr. Pierre Kory in May 2021 then ignored the FLCCC’s dosing recommendations.(9)
WHAT DID WE LEARN FROM PAGE 4?
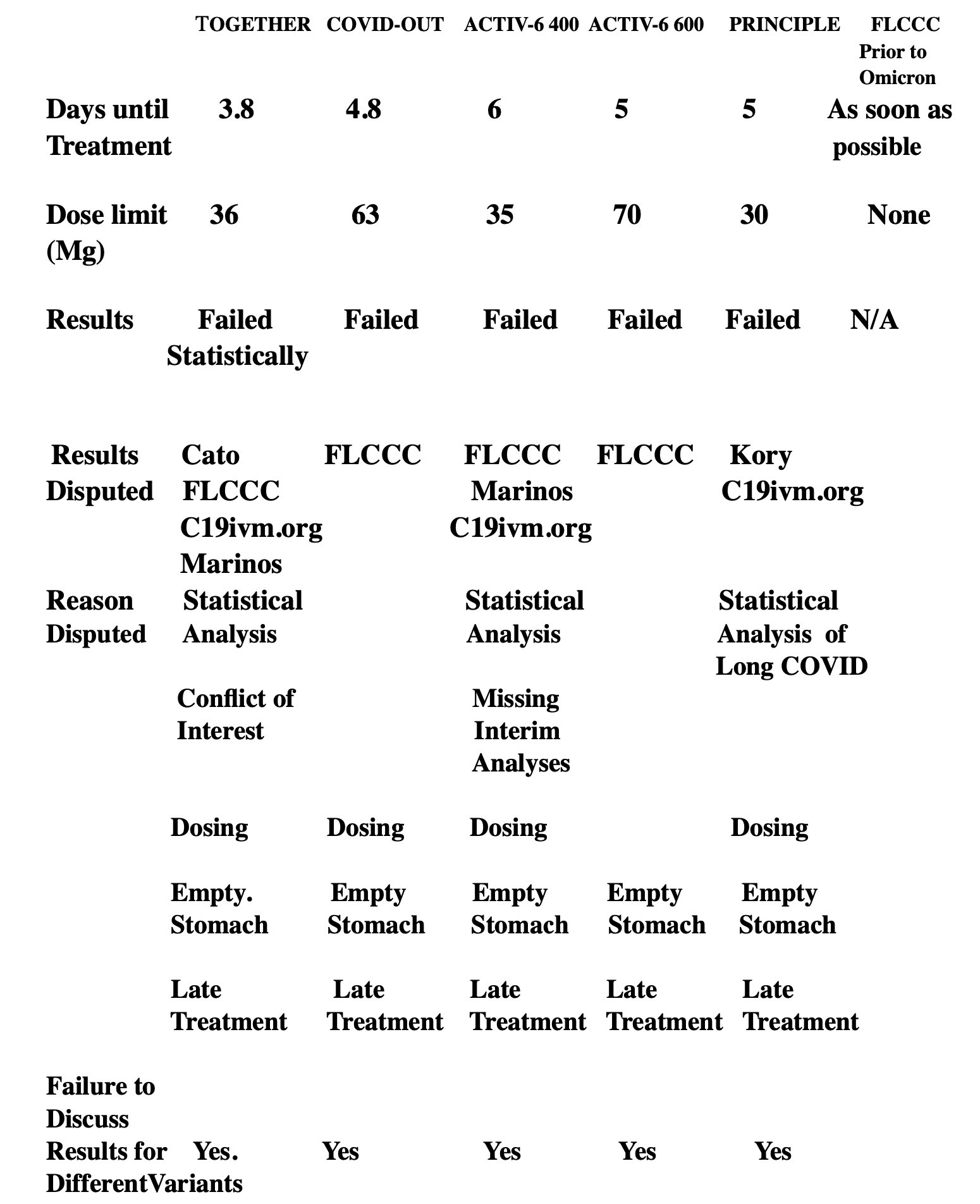
By modern standards ivermectin was given very late in all 5 trials, an average of 4.9 days.
In ACTIV-6 600 which started 2 months into the omicron surge, the placebo group was only sick for an average of 8 days. Patients got ivermectin at a high dose of ivermectin at an average of 5 days into symptoms which is too late for omicron and its descendants Ivermectin has never been given at a reasonable dose, earlier than 5 days into symptoms in a large randomized trial of ivermectin in omicron patients.
TOGETHER, ACTIV-6 400 and PRINCIPLE limited the dose of ivermectin at 90, 90 and 82 kg respectively to 36 mg., 35 mg. And 30 mg. respectively. It meant that overweight patients who were already at higher risk were put at further risk by having their dose limited. COVID-OUT didn’t limit the dose until 160 kg weight and a 63 mg. Ivermectin dose.(10)
All 5 trials declared that ivermectin failed to show statistical benefit.
The results were disputed by the FLCCC Alliance, Dr. Pierre Kory as an individual, Alexandros Marinos, members of the Cato Institute and c19ivm.org
The results were disputed due to severe underdosing, giving ivermectin on an empty stomach, giving it late, failing to report data which would have shown benefit, changing the primary endpoint in the middle of the trial and deceptive statistical analyses.
In TOGETHER, despite ivermectin being severely underdosed and given on a empty stomach, ivermectin lowered the risk of death 12%, needing a ventilator 23% and the risk of needing hospitalization 17%
According to an analysis from the Cato Institute, TOGETHER failed to report that the chance that ivermectin helped: Day 3 viral clearance 78%, hospitalization 91%, Median days of hospitalization 91%, median number of days to death 66% and need for mechanical ventilation 82%(14)(15). The principal investigator Edward Mills had done extensive work for Bill Gates who sponsored the trial. Gates made $500 million on Moderna stock. He’d have made less if ivermectin were proven to be beneficial in TOGETHER.
The PRINCIPLE trial reported ivermectin as ineffective and that it should not be studied again.(20) C19ivm.org and Dr. Pierre Kory reviewed the trial and found the conclusions to be false(16((17). Per c19ivm.org:
“Significantly improved recovery and significantly lower risk of long COVID with ivermectin, despite very late treatment, low-risk patients, and poor administration.
36% lower ongoing persistent COVID-19 specific symptoms, p<0.0001 (details below). The primary recovery outcome shows superiority of ivermectin (probability of superiority > 0.999), missing from the abstract (details below).
The p values for sustained. recovery, early sustained recovery, alleviation of all symptoms, and sustained alleviation are all < 0.0001.
The efficacy seen for ivermectin here is despite the trial being the most clearly designed to fail trial, with major bias in design, operation, analysis, and reporting. This trial is a great example of bias in clinical trials which will be covered in detail in the future.”
10. Let’s talk about the NIH sponsored ACTIV-6 400 trial:
a). The cumulative dose was 39% of that recommended by the FLCCC Alliance. 2nd author, Dr. David Boulware asked Dr. Pierre Kory about dosing 5/27/21 then ignored the FLCCC’s recommendations. He then lied to a Minneapolis Star reporter.(19)
a). It treated patients the latest, 6 days into symptoms. 75% would not have qualified for paxlovid. 25% got the medicine 8 days or later when it was worthless.
b). It included 109 patients who were asymptomatic when they received their medicine and could not get better with treatment.
c). Later we’ll show that ivermectin was beneficial for delta and not omicron. They didn’t report it.
d). The study was supposed to have 1200 patients unless by enrolling more, ivermectin might show benefit for hospitalization or death. The investigators enrolled an extra 391 patients with 95% omicron. By 1200 patients it was obvious that ivermectin, as it was given. was worthless for omicron. The extra 391 patients with almost no benefit were enrolled for the sole purpose of decreasing the benefit of ivermectin overall.
The study should have stopped at 1200 patients. Those 1200 patients showed significant benefit overall because the first 924 patients had over 90% delta and ivermectin was effective for delta.
e). If ivermectin showed benefit at any of the interim analyses every 300 patients, it would be declared effective. ACTIV-6 400 failed to report any of the interim analyses it was supposed to report probably because ivermectin would have shown benefit at 900 and probably 600 patients, overwhelmingly with delta.
f). Not reporting the interim data also meant there was no safety data. The investigators offered an excuse for not reporting the interim data, “ “the rate of enrollment was so rapid, it was not possible to complete the interim analyses’.(13) I don’t know how anyone would have the nerve to put that in print.
g). Ivermectin showed a 98% chance of benefit at the original primary endpoint of 14 days, 97% at 7 days. The whole point of the trial was to see if ivermectin made people get better quicker. Severely underdosed, given on an empty stomach and given very late, it did. The investigators unethically changed the primary endpoint during the trial to 28 days where the chance of benefit was still 91% and declared ivermectin ineffective. Changing the primary endpoint during a trial to intentionally try to make it appear ineffective instead of effective is among the worst kinds of ivestigator fraud. (18)
h). Anyone would gladly have take a cheap, safe drug with a 91% chance of benefit rather than get no treatment.
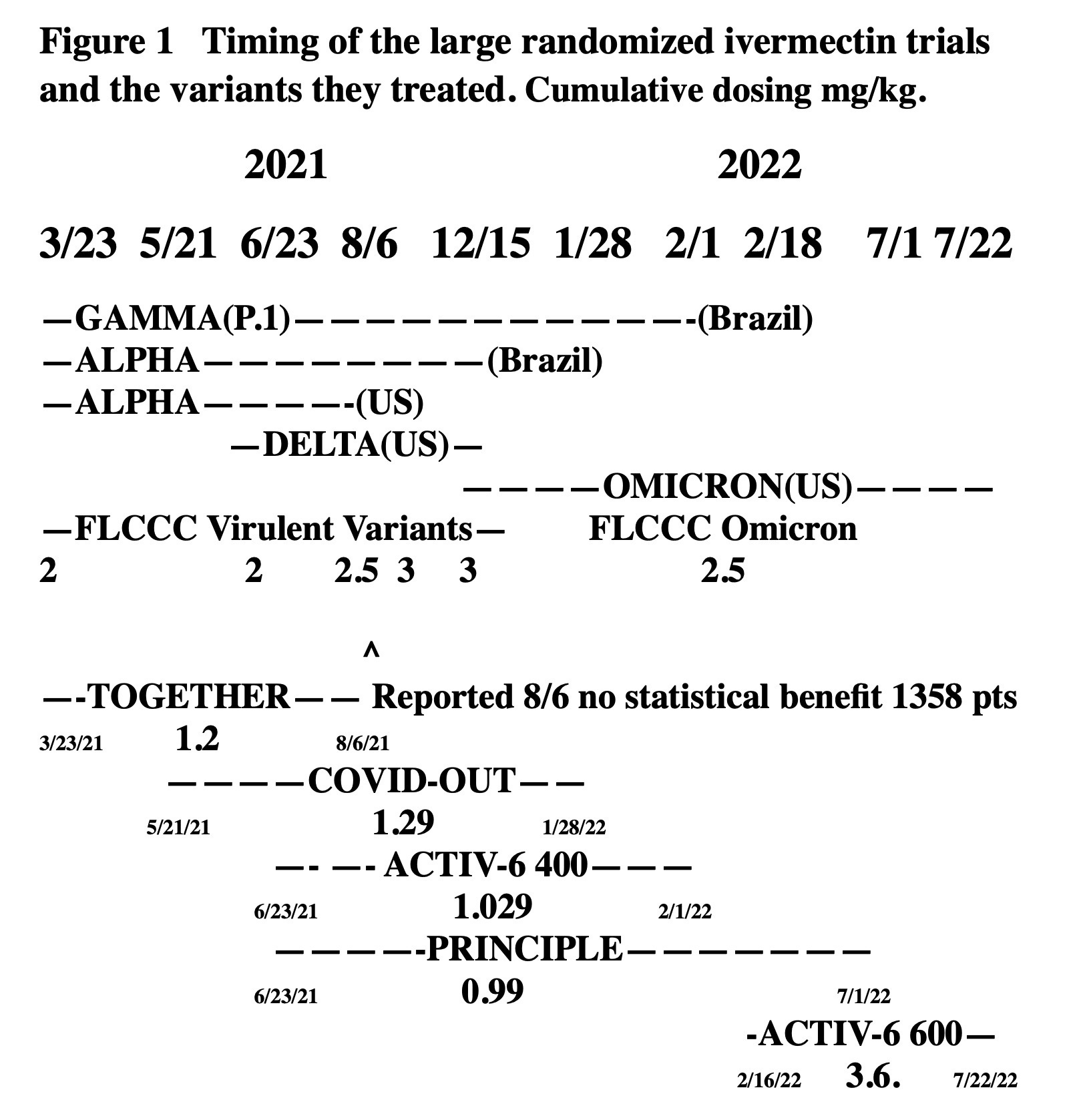
WHAT CAN WE SAY ABOUT THE 4 TRIALS WHICH STARTED PRIOR TO OMICRON?
1). We can see where the 4 trials started prior to when omicron began and the dosing they received.
2). Alpha and the nasty gamma P.1 variant appeared in different parts of Brazil making it hard to evaluate.
3). We have shown that Guzzo et al. showed that ivermectin 120 mg for 3 days was safe and well tolerated. Why did COVID-OUT, ACTIV-6 400 and PRINCIPLE use such low doses. There was a pandemic going on. People were desperate for a treatment. There is lots of other data showing the safety of much higher doses of ivermectin.
4). COVID-OUT, ACTIV-6 400 and PRINCIPLE all had a lot of delta early on which had 1000 times the copies of the Wuhan strain and should have needed a higher dose of ivermectin.
5). When the ACTIV-6 400 trial first enrolled patients 6/23/21, they recommended 0.4 mg/kg on an empty stomach for 3 days. The FLCCC ivermectin experts recommended a 67% higher cumulative dose, giving it for 5 days and with or after a meal.
6). The FLCCC Alliance increased their recommended dose to 0.4-0.6 mg/kg in early August and 0.6 mg/kg in early September based on reports from around the world. Once the trials started the trials couldn’t change their dosing but when it was obvious they had severely underdosed ivermectin, they could have added a high dose arm.
7). ACTIV-6 400 had chosen the same dose as TOGETHER. It meant that if ivermectin failed in TOGETHER, they would be repeating a negative study.
8). 8/6/21 TOGETHER announced that ivermectin failed to show statistical benefit in 1358 patients. ACTIV-6 400 was now treating 96% delta.
Instead of stopping the trial and starting all over again with a much higher ivermectin dose or at the least adding a high dose arm. ACTIV-6 400 enrolled over 1400 more patients to placebo or a LOWER dose of ivermectin that what had failed in TOGETHER.
The only reasonable explanation I can think of was that the investigators wanted ivermectin to fail.
It appears to me that the investigators made choices so that those randomized to ivermectin would get as little benefit as possible in order to make ivermectin appear ineffective. Those who were randomized to ivermectin should be very upset by that.
9). Dr. Francis Collins, chairman of NIH and Cliff Lane deputy chairman of NIAID, WCG IRB, who was supposed to look out for patient safety and the principal investigators of ACTIV-6 400 and COVID-OUT were emailed in Oct 2021 that the US had 99% delta and were giving patients 40% of the FLCCC recommended dose on an empty stomach and the same dose as they were using failed to show statistical benefit in the TOGETHER trial. By then the trial was about 50% enrolled.
The ACTIV group met and considered adding a high dose arm but no changes were made. Those randomized to ivermectin continued to be severely underttreated.
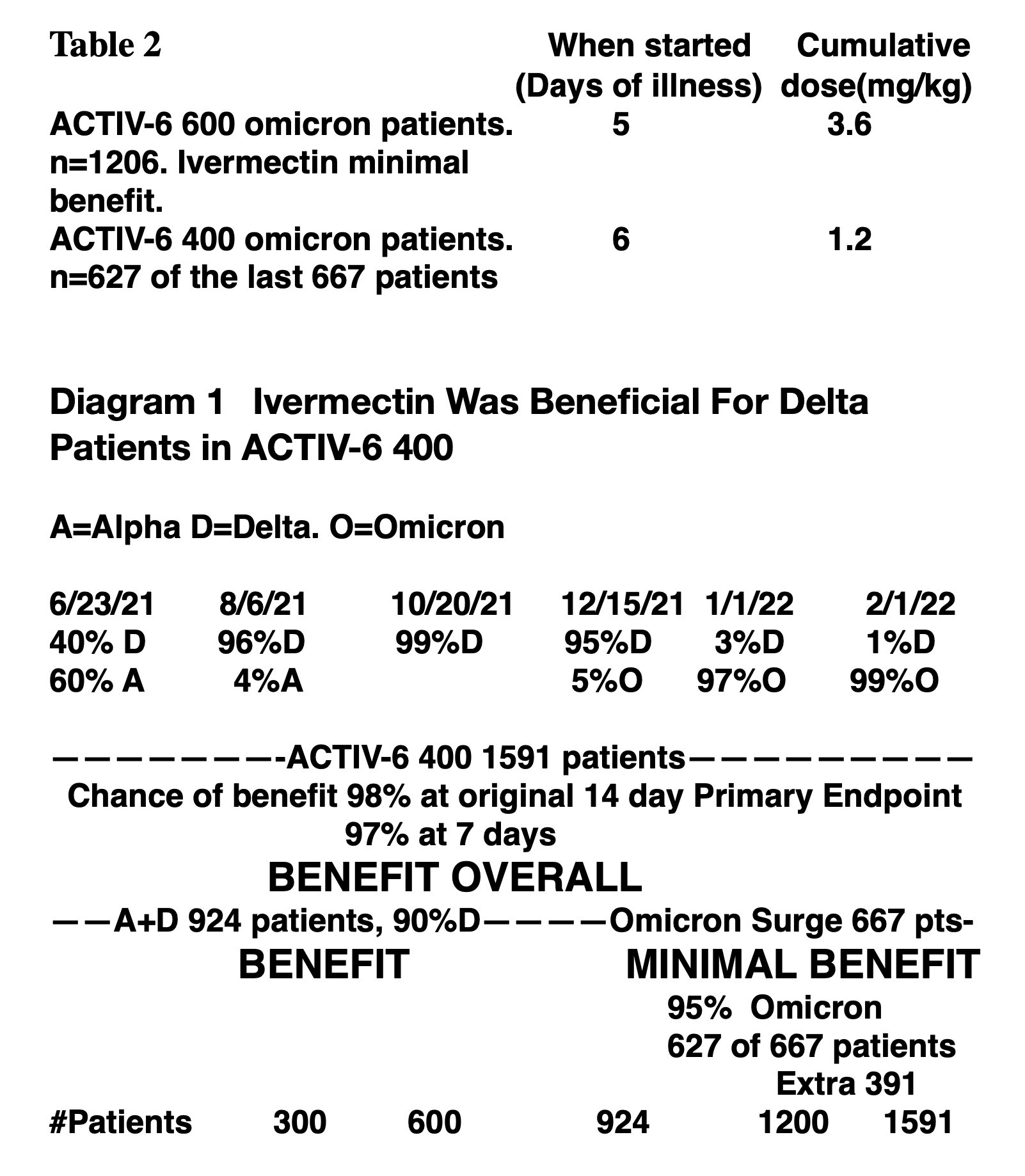
Table 2. (1). In ACTIV-6 600, 95% delta, the patients got a big dose cumulative of ivermectin, 3.6 mg/kg given an average of 5 days into symptoms. Patients got minimal benefit.
(2). In ACTIV-6 400, there were 667 patients in the omicron surge, 95% omicron. Those patients had ivermectin started a day later than those in ACTIV-6 600 and got one third the cumulative dose. Therefore the 95% of those 667 patients with omicron got less benefit from ivermectin than the ivermectin patients in ACTIV-6 600, almost none
(3). Ivermectin showed a 98% chance of benefit at the original primary endpoint for the 1591 patients overall.(12)
(4). We proved that about the 627 of the last 667 patients at the end of the trial had omicron and no benefit.
(5). For ivermectin to have benefit overall in the 1591 patients and have no benefit in 627 of the last 667 patients, the patients prior to that, the 924 patients with over 90% delta had to show benefit.
(6). It means that COVID-OUT, ACTIV-6 400 and TOGETHER each treated over 90% delta cumulatively from mid July 2021 to mid December 2021. Since they were using similar dosing, they had to all have seen benefit for delta in real time and had to have seen the obvious change to no benefit for the omicron patients starting in mid December.
(7). The trials were all in communication. Had they pooled their data and reported it to the public, ivermectin would have been declared effective probably by the end of September 2021 and would have been of great value to the many millions of delta patients until omicron came along.
(8). None of the trials reported having made any attempt to see if the different variants responded differently to ivermectin. We’ll see that it was because ivermectin was beneficial for delta and not omicron as dosed. The trials saw it in real time and would have had to report so they didn’t and lumped everything together.
The NIH ACTIV group knew people were complaining that ivermectin had been underdosed in earlier trials so they ran a 2nd trial, ACTIV-6 600 and renamed the initial trial ACTIV-6 400. They randomized patients to placebo or 0.6 mg/kg for 6 days, 3 times the prior cumulative dose, started an average of 5 days into symptoms. If ivermectin failed to show benefit, allegedly it would prove that ivermectin was ineffective at very high doses. Ivermectin showed little benefit in the trial published in JAMA Network 2/20/23.
At a Higher Dose and Longer Duration, Ivermectin Still Not Effective Against COVID-19(7)
A Cochrane meta-analysis of 11 eligible trials examining the efficacy of ivermectin for the treatment of COVID-19 published through April 2022 concluded that ivermectin has no beneficial effect for people with COVID-19.1
Since May 2022, an additional 3 large randomized clinical trials including several thousand participants have been published, each reaching a similar conclusion.2-4
Today JAMA publishes a new trial of ivermectin treatment for mild to moderate COVID-19 that addresses the possibility that the existing literature may have missed the efficacy of ivermectin because the previously tested dose (approximately 400 μg/kg daily for 3 days) was insufficient.5 At a higher treatment dose (600 μg/kg daily) and longer treatment duration (6 days), Naggie and colleagues again conclude that ivermectin is not beneficial for the treatment of COVID-19.
At the doses and durations tested in these studies, ivermectin does not appear to be associated with serious adverse effects. However, a generally well-tolerated therapy that lacks efficacy can still be dangerous, particularly if it results in patients forgoing other interventions with proven efficacy, such as evidence-based COVID-19 treatments6 or vaccination against SARS-CoV-2. Ivermectin has been used throughout the pandemic.7
Although the current prevalence of ivermectin use in the US and globally is difficult to determine, reports in the lay media as well as our own experience as clinicians suggest that use of ivermectin for COVID-19 has not fully abated, fueled in part by real or perceived lack of access to effective therapies, continued confusion or misinformation, and active disinformation about ivermectin’s efficacy, including by physicians.8
Scientists will continue to produce knowledge on the effectiveness of interventions for the prevention and treatment of COVID-19.9JAMA will continue to vet this science and help disseminate the highest-quality work to clinicians, patients, and the general public.
But closing the knowledge gap is, on its own, not sufficient, and more must be done in partnership with others to address the misinformation that continues as we embark on the fourth year of the COVID-19 pandemic.
Dr. Bibbins-Domingo mentioned that in 3 randomized trials with several thousand patients that ivermectin failed to show benefit. We’ve seen that there were terrible problems in those trials. She mentioned that a Cochrane group analysis showed that ivermectin was ineffective. I’ll show that that analysis was corrupted.
She said that some people had concerns that prior trials failed due to underdosing of ivermectin. They were right. Underdosing was the main reason ivermectin had failed. She went on to say that in ACTIV-6 600 with a higher dose and longer treatment duration of that ivermectin failed to show benefit. Most readers assumed that implied that the ACTIV-6 600 results somehow refuted the arguments that underdosing caused ivermectin to fail. That was what Dr. Bibbins-Domingo wanted readers to think. Her logic was completely wrong.
The ACTIV-6 400 trial had already shown that ivermectin showed a 98% chance of benefit at the original primary endpoint of 14 days. ACTIV-6 600 started ivermectin a day earlier and used a 3 times higher cumulative dose than ACTIV-6 400. You would think ivermectin would show tremendous benefit in ACTIV-6 600 but it showed almost no benefit. How could that be?
The answer is simple. ACTIV-6 600 gave ivermectin to 95% omicron patients at 5 days of symptoms when nothing would work well. The 3 trials, PRINCIPLE, COVID-OUT and ACTIV-6 400 each treated over 90% delta patients over the 5+ months that delta dominated. Over 50% of the patients in ACTIV-6 400 had delta.
I showed that ivermectin had benefit for delta. It’s apples and oranges. ACTIV-6 600 was omicron. ACTIV-6 400 was delta.
The ACTIV-6 600 trial was only done to fake out readers to believe that ivermectin would not have worked at higher doses. ACTIV-6 knew from the last 667 patients in ACTIV-6 400 that ivermectin was worthless for omicron as dosed and would fail in ACTIV-6 600. (6)
Had ivermectin been given to the patients of TOGETHER, COVID- OUT, ACTIV-6 400 AND PRINCIPLE at the dosing used in ACTIV-6 600 or the FLCCC Alliance recommended dosing, ivermectin would have crushed COVID in all the trials and they would have had to stop them all prematurely because of benefit. ACTIV-6 600 and the editorial was a scam.
Ironically, if the ACTIV-6 investigators had not run the ACTIV-6 600 trial, we would never have been able to prove that ivermectin was effective for delta and not omicron in these trials.
Dr. Bibbins-Domingo was not the only one to do a deceptive editorial about the ivermectin trials. On 8/17/22 the New England Journal of Medicine reported the COVID-OUT trial. It was accompanied by an editorial by Drs. Karim and Devnarain, both PhDs, Time to Stop Using Ineffective Drugs.(21)
They demonstrated no knowledge of ivermectin and how it should be used. They didn’t ask the most basic question. Did they use a high enough dose of ivermectin? The New England Journal of Medicine generally refused to publish data the government did not like.
NEJM published TOGETHER and COVID-OUT and JAMA Network published ACTIV-6 400 and ACTIV-6 600. NEJM and JAMA reviewers could not possibly have missed all of the very obvious problems in these trials. The same can be said about the Journal of Infection which published PRINCIPLE.
The Biden administration provided constant pressure on those in medicine not to contradict their statements about repurposed drugs and COVID vaccines.
There was a lot of corruption in some journals and a lot of fear in those who weren’t corrupted. Far more articles were retracted than ever before, generally due to pressure by drug companies and the government. Physicians in the community never got anything close to the truth. Corruption was everywhere, even the Cochrane group, known as the world’s foremost data analysts.
Dr. Bibbins-Domingo mentioned the Cochrane analysis. The Cochrane group is felt to be the most elite data analysts. The Cochrane analysis of 2021 claimed that by reviewing 14 trials it proved that ivermectin was ineffective for prevention, inpatients and outpatients with COVID. She quoted the Cochrane 2022 anlaysis OF 11 trials. There were 3409 patients included in the study including 1358 from the TOGETHER trial which we showed did many unethical things and 400 patients from the JAMA Network published Lopez-Medina trial which 100 physicians demanded be retracted. (22) It is not conceivable that the skilled reviewers of the Cochrane group would not have seen the many serious problems in these trials.
(2). 3/8/24 the Cochrane group published another report on line saying that based on 11 studies with 2860 patients, they concluded again that ivermectin was ineffective for prophylaxis, inpatients and out- patients. They again included Lopez-Medina and TOGETHER, a combined 61% of the patients. None of the trials they reviewed had any omicron patients making the analysis worthless. They did not include any of the 4 most recent large randomized trials with about 6000 patients, about half omicron.
I wrote them and asked them to explain their article. They did not reply until I published an article about it in Trialsite News. They then sent a feeble response a few days later and pulled the article off the internet. There was no way for them to explain their deceptive article. They just assumed everyone would just accept what they said as gospel without analyzing the article. I have a copy of that article.
They were corrupted and got caught. Their 2021, 2022 and 2024 review articles are as deceptive as possible. The details are in my two Trialsite News articles about the Cochrane group.
22 Moderator: Was ivermectin effective in preventing death?
Goodkin: The early randomized trial data and meta analyses showed ivermectin to substantially lower mortality rates. There is science to explain it. There is data from 34 patients with low oxygen saturations that the combination of ivermectin, doxycycline and zinc normalized the oxygen saturations within 24 hours in 61% of the patients, presumably due to the prevention of hemagglutination, clumping of red blood cells.
Academic researchers decided the studies were not of sufficient quality and discounted them. They were a lot better than the dishonest large randomized trials which were subsequently performed.
Moderator: How did hospitalized patients do with ivermectin in US hospitals?
Goodkin: We have no data in the US partly related to the unimaginable actions of the many hospitals who refused to allow ivermectin to be given to many desperately ill patients even when ordered by a physician or requested by the family. Hospitals were willing to fight families in court to prevent dying patients from receiving ivermectin which is very safe and posed no risk. Ivermectin is an FDA approved drug which was being used off label as 20% of all drugs are used.
Attorney Ralph Lorigo in Buffalo represented 200 families who were trying to get ivermectin for their critically ill loved one. He told me that 70 times he won in court. 67 of the 70 lived. 3 patients, all on ventilators for at least a month died. Of the other 130 patients in whom he lost in court or didn’t get to a judge in time, all but one died. That patient’s family lost in the Wisconsin Supreme Court but the family sneaked in ivermectin and the patient lived.
23 Moderator: Who is this video aimed at?
Goodkin: It’s mainly aimed at physicians, the majority of whom have total faith in academic medicine and cannot conceive of the corruption going on. Most physicians I speak to get angry with me when I suggest that academic medicine was corrupted and they refuse to look at my data. One of my doctors started yelling at me in his office. A recent JAMA Network article claimed that Americans’ confidence in physicians has dropped from 71.5% to 40.1%. Many would tell you it is from physicians failing to protect them from the government.
Dr. Pierre Kory has been screaming at the top of his lungs for years about ivermectin fraud and wrote a book about it. War on Ivermectin but most physicians, especially academic physicians, have ignored him. Few physicians have read the large, randomized ivermectin trials or any of the criticisms of the trials. They quote the results of these trials as if the conclusions were handed down by god, never considering that Dr. Kory was right and that some of their fellow academic physician colleagues are among the worst criminals in the history of medicine.
Normally academic physicians go over trials like ACTIV-6 400 with a fine tooth comb and find every problem. In the case of ACTIV-6 400, no one in academic medicine said a word. Most of the serious problems in these trials was very obvious. I sent evidence of the problems to hundreds of academic physicians, including many at Duke which ran ACTIV-6 400 and many involved in the trial. I sent the data showing the problems to all the major physician organizations multiple times. They did nothing. It was mostly out of fear.
Those in academic medicine should realize that if the democrats get voted out they will be able to go back to helping patients instead of helping the government cover up its crimes against humanity,
If any physicians sees this video, I hope they realize that much of the upper echelon of academic medicine has acted unethcally and cowardly, resulting in ivermectin being falsely recommended against for mild to moderate COVID not just for Americans but for the 8 billion people of our planet, causing serious consequences.
Ivermectin can be made in bulk for less than $20 a person while drug company antivirals will never be affordable for the vast majority of the earth’s inhabitants, including many americans.
Moderator: Why do you think no one in academic medicine came forward?
Goodkin: For individuals it was fear of losing their job and career. For institutions it was their share of the $135-178 billion HHS paid out to medical groups during COVID, the fear of losing future funding and fear of being attacked by the federal government and the media.
Moderator: How do you think the public will receive this video?
Goodkin: Many already suspect government corruption and incompetence from the way the vaccines and everything else was handled during the pandemic. Those who had faith in government will realize that the entire medical system acted terribly during COVID.
They would realize that were deceived by a combination of the US government healthcare agencies, those in academic medicine who performed the fraudulent trials, those in the academic medicine who failed to go public with the obvious fraud and the media who ran “hit pieces” on ivermectin instead of doing due diligence on the trials.
Moderator: Do our political leaders know anything about this.
Goodkin: I don’t know. I hope RFK Jr. and Dr. Robert Redfield will see this then bring the truth to all Americans about how ivermectin was sabotaged by the government healthcare agencies, American academic medicine and the media in order to help drug companies make money.
RFK Jr. and Dr. Redfield need to ask the house select subcommittee on the coronavirus pandemic to subpoena the raw data from the ACTIV-6 400 trial so my allegations can be corroborated.
It’s very important that this gets to the physicians in other countries most of whom can’t use ivermectin and many of whom have been punished for using it. Many American physicians have been inappropriately punished for prescribing ivermectin and deserve restitution.
Moderator: Do you expect to be attacked if this gets to the public?
Goodkin: For certain. I’ll be attacked personally as is everyone who contradicts the government’s positions and especially those who allege government fraud. Those involved in the 4 trials will say my analysis is inaccurate and will get prominent people to lie and attest claim that the analysis is wrong but any physician who does due diligence in reviewing the trials and my data will know it is accurate.
I hope that some prominent american physicians who have not been paying attention will see the video, be tremendously disturbed by what happened and will speak up.
If enough physicians see it and corroborate it, they will be calling for the heads of everyone involved in the trial.
Moderator: Do you think the democrats have any idea of what went on?
Goodkin: I have no idea who, if any, among the democrats had any idea of what was going on. You would think that someone knew something. Democrats have done some things which are hard to understand but sabotaging an effective COVID drug to help drug companies make money and harm Americans seems like something no one in leadership would agree to be part of. It is possible that NIH went rogue but it was on the democrats’ watch.
Even if this video does not reach many physicians or many in the public, I hope that lawyers will use it as the basis to seek damages from those involved in ACTIV-6 400 for the Americans damaged by their criminal actions in the ACTIV-6 400 trial. Those involved in COVID-OUT are equally guilty. Hopefully the truth will come out in discovery as I expect many physicians who get sued to look for deals to cover their butts.
Lastly I am hoping that RFK Jr. and Children’s Health Defense are deemed to have standing before the Supreme Court regarding their lawsuit about government censorship. The Supreme Court needs to know that the government is not censoring things they deem “misinformation” because those things are not true or because they are harmful to the country. The government is censoring things because they point to the government’s own unethical behavior in sabotaging effective COVID drugs and promoting dangerous COVID vaccines for the benefit of drug companies and to the detriment of Americans.
References
1. Gilmar Reis, M.D., Ph.D. https://orcid.org/ 0000-0002-4847-1034, Eduardo A.S.M. Silva, M.D., Ph.D. et al. Effect of Early Treatment with Ivermectin among Patients with Covid-19 Published March 30, 2022 N Engl J Med 2022;386:1721-1731 DOI: 10.1056/NEJMoa2115869 VOL. 386 NO. 18
2. Carolyn T. Bramante, M.D., M.P.H. https://orcid.org/ 0000-0001-5858-2080, Jared D. Huling, Ph.D., Christopher J. Tignanelli, M.D. et al. Randomized Trial of Metformin, Ivermectin, and Fluvoxamine for Covid-19 Published August 17, 2022 N Engl J Med 2022;387:599-610
Effect of Ivermectin vs Placebo on Time to Sustained Recovery in Outpatients With Mild to Moderate COVID-19A Randomized Clinical Trial JAMA.10/21//2210/212/2022;328(16):1595-1603. doi:10.1001/ jama.2022.18590
5. Gail Hayward, Ly-Mee Yu, Paul Little et al. Ivermectin for COVID-19 in adults in the community (PRINCIPLE): An open, randomised, controlled, adaptive platform trial of short- and longer- term outcomes
Research Article| Volume 88, ISSUE 4, 106130, April 2024
Ivermectin for COVID-19 in adults in the community ...
6. Michael B. Goodkin MD Why did Cochrane Pull Their Ivermectin Evidence Article Down from the Internet? Trialsite News 7/4/24
At a Higher Dose and Longer Duration, Ivermectin Still Not Effective Against COVID-19. Editor's Note February 20, 2023JAMA. 2023;329(11):897-898. doi:10.1001/jama.2023.1922
8. Guzzo CA, Furtek CI, Porras AG, et al. Safety, tolerability, and pharmacokinetics of escalating high doses of ivermectin in healthy adult subjects. J Clin Pharmacol 2002;42(10): 1122-33
10. Susanna Naggie, MD, MHS1,2; David R. Boulware, MD, MPH3; Christopher J. Lindsell, PhD4; et al for the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV-6) Study Group and Investigators
Effect of Ivermectin vs Placebo on Time to Sustained Recovery in Outpatients With Mild to Moderate COVID-19 A Randomized Clinical Trial. Limitations Section JAMA.10/21//2210/212/2022;328(16):1595-1603. doi:10.1001/ jama.2022.18590
Effect of Higher-Dose Ivermectin for 6 Days vs Placebo on Time to Sustained Recovery in Outpatients With COVID-19A Randomized Clinical Trial. Discussion paragraph 2
JAMA. 2023;329(11):888-897. doi:10.1001/jama.2023.1650 February 20, 2023
13. Susanna Naggie MD MHS; David R. Boulware, MD, MPH3; Christopher J. Lindsell, PhD4; et al for the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV-6) Study Group and Investigators
Effect of Ivermectin vs Placebo on Time to Sustained Recovery in Outpatients With Mild to Moderate COVID-19A Randomized Clinical Trial ACTIV-6 supplemental data 3 Independent Data Monitoring Oversight page 9
18. Hooper, C, Henderson DR, Cato Institute: Ivermectin and Statistical Significance At what point should a potential therapy be deemed effective? Spring 2022 • Regulation
20. Nuffield Department of Primary Care Health Sciences : Medical sciences division. “New study shows ivermectin lacks meaningful benefits in COVID-19 treatment”
21. Salim S. Abdool Karim, M.B., Ch.B., Ph.D., and Nikita Devnarain, Ph.D Time to Stop Using Ineffective Covid-19 Drugs Published August 17, 2022 N Engl J Med 2022;387:654-655 DOI: 10.1056/NEJMe2209017 VOL. 387 NO. 7
23. Lawrence B. Afrin MD et al. Covid-19 hyperinflammation and post-Covid-19 illness may be rooted in mast cell activation syndrome Int J Infect Dis 2020 Nov:100:327-332. doi: 10.1016/j.ijid.2020.09.016. Epub 2020 Sep 10.
24. Christina M. Brennan et al. Oral famotidine versus placebo in non-hospitalised patients with COVID-19: a randomised, double-blind, data-intense, phase 2 clinical trial https://doi.org/10.1136/gutjnl-2022-326952
Until doctors start caring about this sort of thing, their patients won't.
I know quite a few people-- mostly older and well educated--that treat their doctors like a god. Until Dr. God says do it, they won't, and won't pay attention to anything that is contrary to Dr. God.
Using less than a clinically effective dose is a typical trick of NIH. NIH does these "setup-to-fail" research studies to fool Congress, State-Controlled-Media, and others that NIH has "studied this drug and found it to be ineffective." I received $$Millions of NIH funding, and knew how to play their game.





















Until doctors start caring about this sort of thing, their patients won't.
I know quite a few people-- mostly older and well educated--that treat their doctors like a god. Until Dr. God says do it, they won't, and won't pay attention to anything that is contrary to Dr. God.
Using less than a clinically effective dose is a typical trick of NIH. NIH does these "setup-to-fail" research studies to fool Congress, State-Controlled-Media, and others that NIH has "studied this drug and found it to be ineffective." I received $$Millions of NIH funding, and knew how to play their game.