


LONG COVID Research = COVID-19 Vaccine Injury Research (except for Turbo Cancer!) - Eric Topol's Fraud (I dissect the largest review paper on Long COVID published Jan.2023)

The Medical Industrial Complex is an iatrogenic profit generating monster which just so happens to be the third-leading cause of death in America. When factoring the society-wide Modified mRNA “vaccine” adverse events, it is highly likely that “medical errors” are the now first and foremost leading cause of death in America, and beyond.
Given the raging “vaccine” induced turbo cancer epidemic currently underway, it would be counterintuitive, more at criminal, for the various medical associations to recommend diets high in sugar (i.e. cancer food), and yet that is precisely what is being advocated for; to wit:

The above advice is literally medical malpractice.
Imagine consuming 25 grams of added sugar per day while concurrently dealing with “vaccine” caused chronic inflammation, p53 protein suppression (which in turn suppresses cancer), and a whole host of other adverse reactions that the walking spike protein factories (i.e. the “vaccinated”) are suffering from…
…and then deceptively label all of these slow kill bioweapon ailments as “Long Covid” while pushing the USDA’s, FAO’s and WHO’s crimes against health Food Pyramid comprised of mostly processed foods high in carbohydrates and sugars; in other words, slowly and not so slowly murdering innocents with genetically modifying “Trust the Science” perma-emergency EUA “treatments” while aggressively promoting poisonous diets.
It is no coincidence that cancer patients are fed a diet of applesauce (pure sugar), crackers (processed white flour that converts to sugar), overcooked vegetables (dead food), and overcooked proteins (low nutrient-dense food) in hospitals. And if the likes of Bill Gates get their way, then bug gruel and tumorigenic synthetic meats will be the primary proteins in hospitals.
The Medical Industrial Complex has cooked up their “Long Covid” coverup scam as their latest alibi, knowing full well that the combination of “vaccines” and their health inversion diets are the driving forces behind “Long Covid.”

Fig. 1: Long COVID symptoms and the impacts on numerous organs with differing pathology.
Source: 2023 Jan (Eric Topol et al) - Long COVID: major findings, mechanisms and recommendations
65 million individuals worldwide estimated to have Long COVID
>200 symptoms identified
Long COVID: 10-30% of non-hospitalized cases, 50-70% of hospitalized cases
“highest % of diagnoses ages 36-50 years old, most long COVID cases are in non-hospitalized patients with mild acute illness”
Hundreds of biomedical findings have been documented, with many patients experiencing dozens of symptoms across multiple organ systems
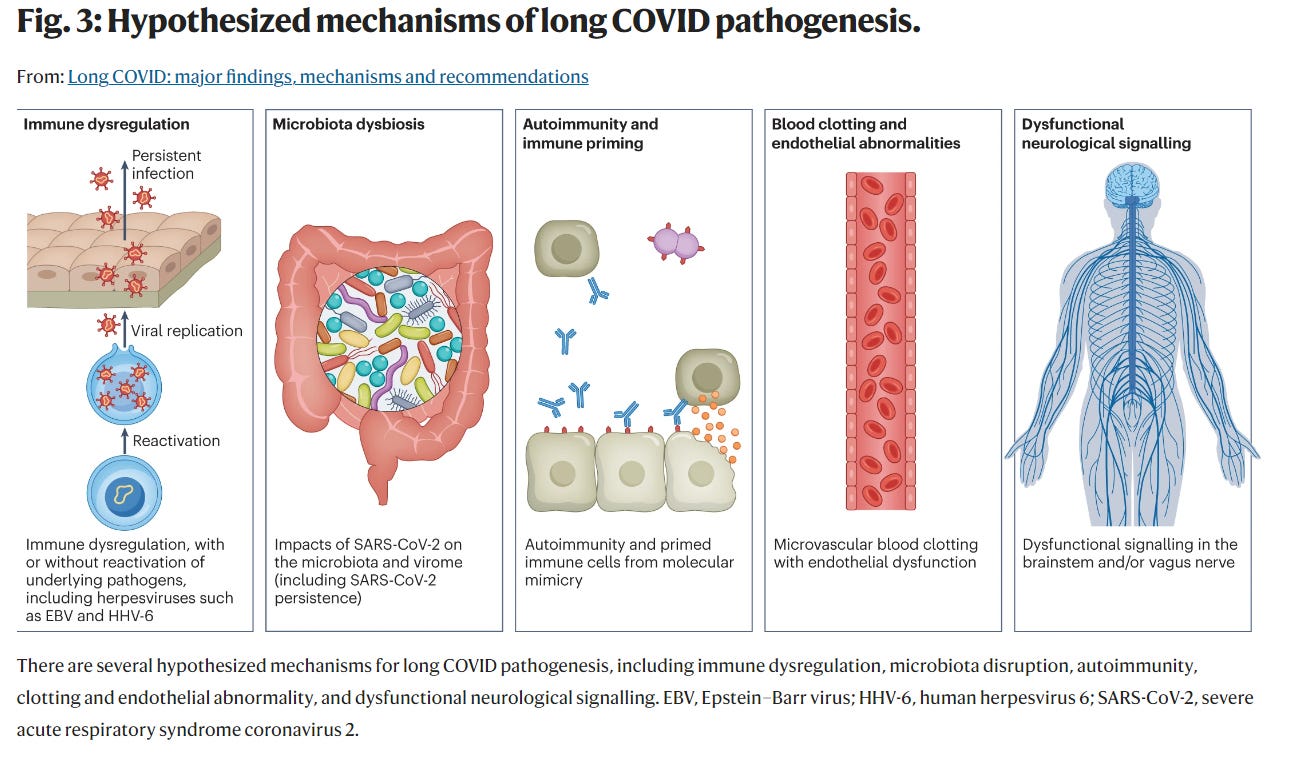
Causes of Long COVID:
1. persisting reservoirs of SARS-CoV-2 in tissues
2. Immune dysregulation
3. Reactivation of viruses like EBV, herpesvirus
4. Impact of SARS-CoV-2 on microbiota
5. Autoimmunity
6. microvascular blood clotting with endothelial dysfunction
7. dysfunctional signalling in brainstem, vagus nerve
Risk Factors: being a woman, Type 2 diabetes, EBV reactivation, autoantibodies, connective tissue disorders, ADHD, allergies
Immune System Damage
exhausted T-cells
reduced CD4+ and CD8+ T-cell numbers
various cytokine abnormalities
high levels of various auto-antibodies, including against tissues (connective tissue, extracellular matrix components, vascular endothelium, coagulation factors and platelets), organ systems (including the lung, central nervous system, skin and gastrointestinal tract)
reactivated viruses including EBV and human herpesvirus 6 (seen in ME/CFS) and lead to mitochondrial fragmentation and severely affect energy metabolism.
EBV reactivation associated with fatigue & neurocognitive dysfunction
Vascular and Cardiac Damage
endothelial dysfunction
deep vein thrombosis, pulmonary embolism, bleeding events
microclots
long lasting-reduction in vascular density mainly affecting small capillaries
Long-term changes to the size and stiffness of blood cells
CARDIAC:
Increased risk of a variety of cardiovascular diseases, including heart failure, dysrhythmias and stroke
Cardiac MRI studies revealed cardiac impairment in 58% of Long COVID
60-70% have single organ damage, 25-30% have multi-organ damage
Increased risk of Type 2 Diabetes
NEURO
memory loss, cognitive impairment, paresthesia, dizziness and balance issues, sensitivity to light and noise, loss of (or phantom) smell or taste, and autonomic dysfunction
tinnitus, hearing loss and vertigo
fatigue was found in 32% and cognitive impairment was found in 22%
Mechanisms of injury:
neuroinflammation
damage to blood vessels & endothelial dysfunction
peptides that self-assemble into amyloid clumps
brain and brainstem hypometabolism
microglial reactivity similar to that seen in chemotherapy, known as ‘chemo-brain’
myelin loss
eyes: impaired retinal microcirculation
low blood cortisol levels
ME/CFS, Dysautonomia
Myalgic encephalomyelitis/chronic fatigue syndrome - multisystem neuroimmune illness
Up to 75% of people with ME/CFS cannot work full-time and 25% have severe ME/CFS, which often means they are bed-bound, have extreme sensitivity to sensory input and are dependent on others for care
Criteria: “substantial reduction or impairment in the ability to engage in pre-illness levels of occupational, educational, social, or personal activities” for at least 6 months, accompanied by a profound fatigue that is not alleviated by rest, along with postexertional malaise, unrefreshing sleep and cognitive impairment or orthostatic intolerance (or both)
Up to 50% of Long COVID people are estimated to meet criteria for ME/CFS
majority of Long COVID experience postexertional malaise
ME/CFS Findings:
exhausted T cells
mitochondrial dysfunction
vascular and endothelial abnormalities including deformed red blood cells
abnormal metabolic profiles
neuroinflammation, reduced cerebral blood flow, brainstem abnormalities
reactivated EBV, human herpesvirus 6, CMV
microclots, hyperactivated platelets
commonly with dysautonomia, POTS, MCAS (Mast Cell Activation Syndrome), Ehlers-Danlos syndrome, endometriosis
REPRODUCTIVE
menstrual alterations
declined ovarian reserve
erectile dysfunction
impairments to sperm count, semen volume, sperm motility and morphology
RESPIRATORY
Shortness of breath in 40% and chronic cough in 20%
lung perfusion abnormalities (microclots)
epithelial damage in the airways
GASTRO
gut microbiota dysbiosis (significantly altered)
specific gut pathogens can cause neurological or respiratory symptoms
Diagnosis
very few good tests available for Long COVID
Cardiac MRI for cardiovascular impairment
trivia: dogs can identify individuals with Long COVID from sweat samples
Treatments
IVIG for immune dysfunction
low dose naltrexone for neuroinflammation
beta blockers, increased salt intake for POTS
famotidine for MCAS
elimination diets for GI symptoms
Who is the Senior Author Dr.Eric Topol?
Dr.Eric Topol is one of the most aggressive pushers of COVID-19 mRNA Vaccines and one of the biggest deniers of mRNA Vaccine injuries today.
He has recently received $282 million research funding from NIH
He is a medical con artist, a fraud, a big pharma sales rep

My Take…
This is a MAJOR review paper on Long COVID. It has many problems which can be summed up as: it’s a fraud. This paper is a fraud.
This is a paper on COVID-19 Vaccine Injuries, re-labeled as “Long COVID”.
It has 210 references. The problem with these 210 Long COVID papers is that none of them account for COVID-19 Vaccine status of the participants and the possibility of vaccine injury.
The moment you ignore COVID-19 Vaccine status of your study participants, your study is null and void, and you’ve committed scientific fraud.
Most of the “causes of Long COVID” proposed by Topol are themselves COVID-19 Vaccine injuries (immune dysregulation, viral reactivation, microbiome dysfunction, autoimmunity, microclots, endothelial dysfunction).
Topol does not recognize Spike protein injury or “spikeopathy”. The spike protein is mentioned only twice in the entire study:
In one study, circulating spike was found in 60% of long COVID patients which Topol explains as “likely implying a reservoir of active virus” (even though they were vaccinated)
SARS-CoV-2 spike protein has been found in central nervous system
So out of 210 papers on Long COVID, Topol makes no connection to spike protein toxicity (for which there are over 3400 peer-reviewed papers, according to Dr.Peter McCullough)
So what plausible causes of Long COVID does Topol propose? Persisting SARS-CoV-2 reservoirs in certain locations like the GI tract. Everything else can be explained by COVID-19 Vaccine Adverse reaction.
Every clinical manifestation of “Long COVID” in this paper is a well known COVID-19 Vaccine Injury.
Interestingly, cancer is not mentioned once in this paper. That suggests to me that Turbo Cancers will ultimately not be blamed on Long COVID but will be blamed on something else.
HARVARD Oncologist Dr. Kimmie Ng already has a theory, in the Feb.6, 2024 story: “Cancer keeps coming for the young. Why?”:
“The main hypothesis is that some not-as-yet-identified environmental exposure is affecting individuals, starting in early life.” - Dr.Kimmie Ng MD MPH, Associate Chief Division of Gastrointestinal Oncology at Dana-Farber Cancer Institute

CONCLUSION:
In the coming weeks and months I am going to dissect the “Long COVID” literature.
But the best way to approach these papers is to try to learn from them, just replace “Long COVID” with “COVID Vaccine Injury”.
I’ve learned a number of things from this paper about the COVID Vaccine Injured who believe they have Long COVID:
highest % of diagnoses in ages 36-50 years old
up to 60% may have abnormalities on Cardiac MRI
Virus reactivation, like EBV, or herpes, is a major problem
gut microbiota dysfunction is a major problem and can cause neurological or respiratory symptoms
mitochondrial dysfunction is a major problem
immune system dysfunction and damage is very severe (impaired immune cells, altered cytokines, auto-antibodies, etc)
30% have fatigue, 20% have cognitive impairment
Up to 50% are estimated to meet criteria for ME/CFS (chronic fatigue syndrome)
majority experience postexertional malaise
chronic shortness of breath, cough can be due to microclots, capillary damage, airway damage
impairments to sperm count, semen volume, sperm motility and morphology
dogs can identify you from sweat samples
The “Long Covid” cure is quite simple actually: stay away from any and all vaccines, limit exposure to any and all environmental toxins, clean up your diet, and administer the correct treatments (especially for turbo cancers) like Ivermectin and Fenbendazole both prophylactically and if you are sick.
And a most germane article from last year also featuring Dr. Makis discussing the parabolic rise in (turbo) cancers:
Oncologist: "I've Never Seen Cancers Behaving Like This"

This Substack has been exposing the DEATHVAX™-induced turbo cancer and all cause mortality surges for well over a year: The latest testimony comes courtesy of Dr. Makis, who explained that young people in their 20s, 30s, and 40s are developing aggressive turbo cancers:
They want you dead.
Do NOT comply.














I would like others to check this out to see how widespread. I recently had a cardiologist appointment to try to determine how much permanent damage was done by the myocardititis I got in February 2021 from my first moderna vaccine. 4 weeks of chest pain and extreme fatigue etc. Anyway when I got my receipt It was coded as "long covid". I do not have long covid. My shot happened a year before I even got my very quick case of covid that was over in 36 hours with early drugs and the correct protocol. I asked the secretary about that and she explained that there is "no code for vaccine injury" so they have to code it long covid. This is outrageous. This happened to me in the US in Texas. Is this universal around the US? What a scam but not surprising. I am medicare age and wondering if this is happening everywhere.
I am a retired RN. Years ago the father of the guy I was dating had bypass surgery and I flew in the help with the recovery process. He was in his 60’s, and a diabetic. The snack they gave him to control his sugar was nilla wafers. I shit you not. I pushed back with the hospital dietitian (who wanted none of what I was selling) and was told later I thoroughly embarrassed the family. No mention of vit D, did I mention he was a black man? Everyone is so afraid to advocate for themselves...we wouldn’t want to hurt feelings because after all, these people are the experts...right? This is why I no longer have anything to do with allopathic medicine. Gave up my license and bought a farm so I can grow/raise as much of my own food as possible. Be your own advocate!!
Oh, and I just did a course of IVM/Fenbendazole and the rest of the protocol as a preventative and possible help with Lyme. Thanks for all the info